|
Dr. Rhonda Patrick discusses the differences between different forms of DHA in terms of bioavailability and transport into different cells. She talks about why a specific type of DHA (DHA in phosphatidylcholine) is more readily transported into the brain because it forms DHA-lysophsophatidylcholine. Krill oil and salmon roe both have a slightly higher concentration of DHA-lysophosphatidylcholine. She also talks about astaxanthin, a carotenoid that is unique to krill oil, and has potent antioxidant activity and prevents the oxidation of DHA and EPA.
0 Comments
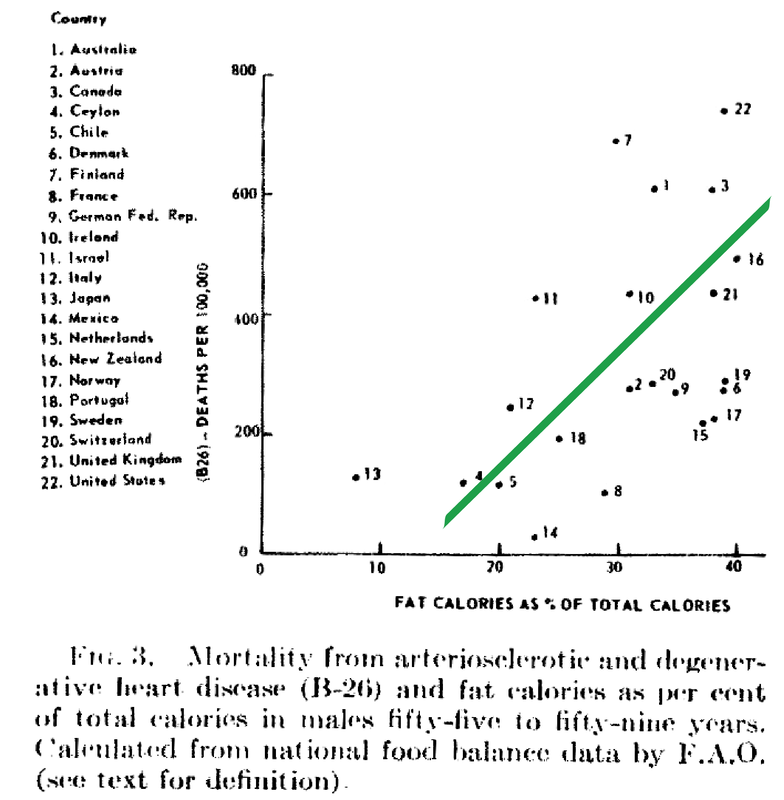
Despite food manufacturers claiming that refined vegetable oils were healthy, Americans experienced an up-rise in heart disease during the early 20th century. Like many new inventions, few questions were initially posited. Unfortunately, an alternate nutrient took the blame due to the research of a single scientist. In 1951, American physiologist and professor Ancel Keys went to Europe in search of the cause of cardiovascular disease. In his quest, he went to observe the eating habits of individuals living Naples, Italy due to reports of a low prevalence of heart disease. During this time, post-war conditions resulted in finite and unusual circumstances in regards to agriculture and infrastructure. Therefore what Keys perceived as a cultural tradition was dubbed the "Mediterranean diet". Keys observed the residents in Naples consumed primarily pasta and plain pizza, with vegetables, olive oil, cheese, fruit for dessert, a moderate amount of wine, and very little meat (except among individuals belonging to a higher socioeconomic status).  Through an informal study measuring cholesterol serum levels among Rotary club members (those who could not afford meat, but could afford cheese) conducted by Keys's wife, whom at the time was a medical technologist, Keys deduced that avoiding meat resulted in a lower incidence of heart attacks. Ancel Keys continued on his biased search for proof that a diet high in saturated fat is correlated with a higher risk of cardiovascular disease. He eventually compiled data from six more countries with high rates of heart disease and diets typically high in saturated fat. At first glance, Keys's research seemed logical and compelling. The evidence was based on the premise that individuals in America, who consumed high amounts of saturated fat, died from heart disease at a higher rate than individuals in Japan, who consumed low amounts of saturated fat.
Unfortunately, Keys had gained the interest of people in positions of power. Upon President Eisenhower's heart attack in 1955, Keys proposed his theory to the president's primary care physician, Paul Dudley White. Days following, White began to advise to the public to reduce the consumption of saturated fat and cholesterol in an effort to prevent cardiovascular disease. Through his connections and influence, Keys soon joined the nutrition committee of the American Heart Association (AHA) which, based on Keys's research, released a report in 1961 that advised patients with a high risk of cardiovascular disease to reduce their consumption of saturated fat. (Interestingly enough, the AHA began its rise to prominence in 1948, the same year Proctor & Gamble donated over $1.7 million to the organization - resulting in the AHA indebted to Crisco.) In 1961, Time magazine placed Ancel Keys on the front cover touting him as "the twenthiest century's most influential nutrition expert." By 1970, Keys published the Seven Countries Study, which detailed his original research - this study has now been cited in over a million other scientific publications. While Keys associative observations between saturated fat and cardiovascular disease never proved causation, he had won the battle of public opinion. With the help of Ancel Keys, the American medical community and mainstream media has advised consumers to stop eating the animal products that have been consumed for centuries, replacing them with bread, pasta, margarine, low-fat dairy, and vegetable oil. This was the dietary shift that was codified by the United States government in the late 1970s. References Central Committee for Medical And Community Program of the American Heart Association. (1961). Dietary Fat and Its Relation to Heart Attacks and Strokes. Circulation [online] 23, pp.133-36. Available at: https://circ.ahajournals.org/content/circulationaha/23/1/133.full.pdf [Accessed 26 Jan. 2019]
Keys, A. (1953). Atherosclerosis: A Problem in Newer Public Health. Journal of Mt. Sinai Hospital, [online] 20(2), pp.118-39. Keys, A. (1970). Coronary Heart Disease in Seven Countries. Circulation. 41 (1), pp.1186-95. Keys, A. (1995). Mediterranean Diet and Public Health: Personal Reflections. American Journal of Clinical Nutrition, [online] 61 (6), pp.1321S-1323S. Available at: https://dx.doi.org/10.1093/ajcn/61.6.1321s [Accessed 26 Jan. 2019] Marvin, H. (1964). The 40 Year War on Heart Disease. New York: American Heart Association. Mercola, J. (2017). Fat For Fuel. Carlsbad, California: Hay House. Teichholz, N. (2014). The Big Fat Surprise. New York: Simon & Schuster, pp.32-33.
The Prospective Urban Rural Epidemiology (PURE) study is a large, epidemiological study that included more than 135,000 individuals between the ages of 35–70 years across 18 countries. Regions included Canada, Sweden, United Arab Emirates, Argentina, Brazil, Chile, China, Colombia, Iran, Malaysia, occupied Palestinian territory, Poland, South Africa, Turkey, Bangladesh, India, Pakistan, and Zimbabwe. Overall, the researchers found that high carbohydrate intake (more than 60% of energy) was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke. For decades, dietary guidelines have focused on reducing total fat and saturated fatty acid intake, based on the presumption that replacing saturated fatty acids with carbohydrate and unsaturated fats will lower LDL cholesterol and should therefore reduce cardiovascular disease events. This focus is largely based on selective emphasis on some observational and clinical data, despite the existence of several randomized trials and observational studies that do not support these conclusions. Results of the Study After documenting 5796 deaths and 4784 major cardiovascular disease events and running statistical analyses, the researchers observed:
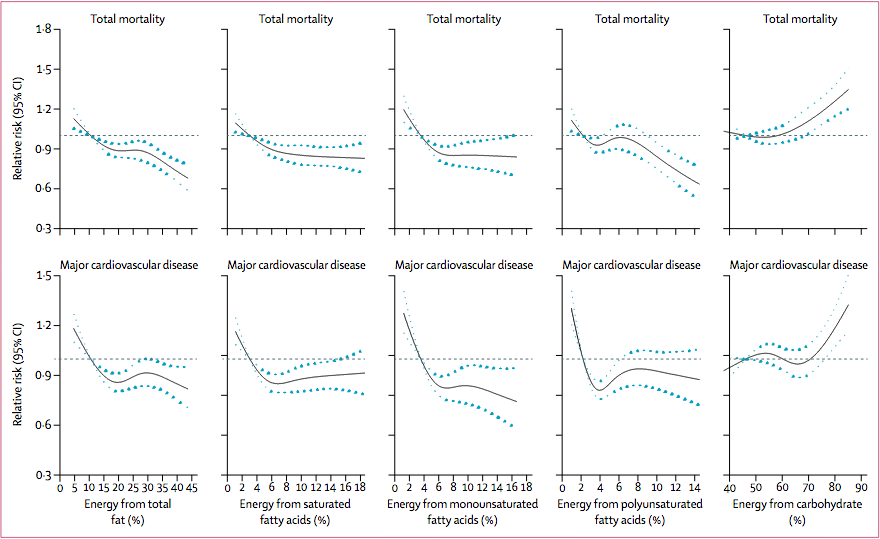 Association between estimated percentage energy from nutrients and total mortality and major cardiovascular disease (n=135335). Image from (Dehghan et al., 2017) Recommendations and Take Away The results of this study do not suggest a low-carbohydrate diet, but rather that a total fat intake of about 35% of energy while lowering carbohydrate intake might lower risk of total mortality. Collectively, the data does not support the recommendation to limit saturated fatty acids to less than 10% of intake and that a very low intake (ie, below about 7% of energy) might even be harmful. Limitations of the Study
The researchers declare no conflicts of interests References Brown, E. (2017). More Evidence That Everything the Government Teaches Us About Eating Is Wrong. [online] Reason.com. Available at: http://reason.com/blog/2017/08/30/pure-study-challenges-dietary-dogma [Accessed 20 Sep. 2017].
Dehghan, M., Mente, A., Zhang, X., Swaminathan, S., Li, W., Mohan, V., Iqbal, R., Kumar, R., Wentzel-Viljoen, E., Rosengren, A., Amma, L., Avezum, A., Chifamba, J., Diaz, R., Khatib, R., Lear, S., Lopez-Jaramillo, P., Liu, X., Gupta, R., Mohammadifard, N., Gao, N., Oguz, A., Ramli, A., Seron, P., Sun, Y., Szuba, A., Tsolekile, L., Wielgosz, A., Yusuf, R., Hussein Yusufali, A., Teo, K., Rangarajan, S., Dagenais, G., Bangdiwala, S., Islam, S., Anand, S., Yusuf, S., Diaz, R., Orlandini, A., Linetsky, B., Toscanelli, S., Casaccia, G., Cuneo, J., Rahman, O., Yusuf, R., Azad, A., Rabbani, K., Cherry, H., Mannan, A., Hassan, I., Talukdar, A., Tooheen, R., Khan, M., Sintaha, M., Choudhury, T., Haque, R., Parvin, S., Avezum, A., Oliveira, G., Marcilio, C., Mattos, A., Teo, K., Yusuf, S., Dejesus, J., Agapay, D., Tongana, T., Solano, R., Kay, I., Trottier, S., Rimac, J., Elsheikh, W., Heldman, L., Ramezani, E., Dagenais, G., Poirier, P., Turbide, G., Auger, D., De Bluts, A., Proulx, M., Cayer, M., Bonneville, N., Lear, S., Gasevic, D., Corber, E., de Jong, V., Vukmirovich, I., Wielgosz, A., Fodor, G., Pipe, A., Shane, A., Lanas, F., Seron, P., Martinez, S., Valdebenito, A., Oliveros, M., Wei, L., Lisheng, L., Chunming, C., Xingyu, W., Wenhua, Z., Hongye, Z., Xuan, J., Bo, H., Yi, S., Jian, B., Xiuwen, Z., Xiaohong, C., Tao, C., Hui, C., Xiaohong, C., Qing, D., Xiaoru, C., Qing, D., Xinye, H., Bo, H., Xuan, J., Jian, L., Juan, L., Xu, L., Bing, R., Yi, S., Wei, W., Yang, W., Jun, Y., Yi, Z., Hongye, Z., Xiuwen, Z., Manlu, Z., Fanghong, L., Jianfang, W., Yindong, L., Yan, H., Liangqing, Z., Baoxia, G., Xiaoyang, L., Shiying, Z., Rongwen, B., Xiuzhen, T., Dong, L., Di, C., Jianguo, W., Yize, X., Tianlu, L., Peng, Z., Changlin, D., Ning, L., Xiaolan, M., Yuqing, Y., Rensheng, L., Minfan, F., Jing, H., Yu, L., Xiaojie, X., Qiang, Z., Lopez-Jaramillo, P., Lopez, P., Garcia, R., Jurado, L., Gómez-Arbeláez, D., Arguello, J., Dueñas, R., Silva, S., Pradilla, L., Ramirez, F., Molina, D., Cure-Cure, C., Perez, M., Hernandez, E., Arcos, E., Fernandez, S., Narvaez, C., Paez, J., Sotomayor, A., Garcia, H., Sanchez, G., David, T., Rico, A., Mony, P., Vaz, M., Bharathi, A., Swaminathan, S., Kurpad, K., Jayachitra, K., Kumar, N., Hospital, H., Mohan, V., Deepa, M., Parthiban, K., Anitha, M., Hemavathy, S., Rahulashankiruthiyayan, T., Anitha, D., Sridevi, K., Gupta, R., Panwar, R., Mohan, I., Rastogi, P., Rastogi, S., Bhargava, R., Kumar, R., Thakur, J., Patro, B., Lakshmi, P., Mahajan, R., Chaudary, P., Kutty, V., Vijayakumar, K., Ajayan, K., Rajasree, G., Renjini, A., Deepu, A., Sandhya, B., Asha, S., Soumya, H., Kelishadi, R., Bahonar, A., Mohammadifard, N., Heidari, H., Yusoff, K., Ismail, T., Ng, K., Devi, A., Nasir, N., Yasin, M., Miskan, M., Rahman, E., Arsad, M., Ariffin, F., Razak, S., Majid, F., Bakar, N., Yacob, M., Zainon, N., Salleh, R., Ramli, M., Halim, N., Norlizan, S., Ghazali, N., Arshad, M., Razali, R., Ali, S., Othman, H., Hafar, C., Pit, A., Danuri, N., Basir, F., Zahari, S., Abdullah, H., Arippin, M., Zakaria, N., Noorhassim, I., Hasni, M., Azmi, M., Zaleha, M., Hazdi, K., Rizam, A., Sazman, W., Azman, A., Khatib, R., Khammash, U., Khatib, A., Giacaman, R., Iqbal, R., Afridi, A., Khawaja, R., Raza, A., Kazmi, K., Zatonski, W., Szuba, A., Zatonska, K., Ilow, R., Ferus, M., Regulska-Ilow, B., Rózanska, D., Wolyniec, M., Alkamel, Ali, M., Kruger, M., Voster, H., Schutte, A., Wentzel-Viljoen, E., Eloff, F., de Ridder, H., Moss, H., Potgieter, J., Roux, A., Watson, M., de Wet, G., Olckers, A., Jerling, J., Pieters, M., Hoekstra, T., Puoane, T., Igumbor, E., Tsolekile, L., Sanders, D., Naidoo, P., Steyn, N., Peer, N., Mayosi, B., Rayner, B., Lambert, V., Levitt, N., Kolbe-Alexander, T., Ntyintyane, L., Hughes, G., Swart, R., Fourie, J., Muzigaba, M., Xapa, S., Gobile, N., Ndayi, K., Jwili, B., Ndibaza, K., Egbujie, B., Rosengren, A., Boström, K., Gustavsson, A., Andreasson, M., Snällman, M., Wirdemann, L., Oguz, A., Imeryuz, N., Altuntas, Y., Gulec, S., Temizhan, A., Karsidag, K., Calik, K., Akalin, A., Caklili, O., Keskinler, M., Erbakan, A., Yusufali, A., Almahmeed, W., Swidan, H., Darwish, E., Hashemi, A., Al-Khaja, N., Muscat-Baron, J., Ahmed, S., Mamdouh, T., Darwish, W., Abdelmotagali, M., Awed, S., Movahedi, G., Hussain, F., Al Shaibani, H., Gharabou, R., Youssef, D., Nawati, A., Salah, Z., Abdalla, R., Al Shuwaihi, S., Al Omairi, M., Cadigal, O., Alejandrino, R., Chifamba, J., Gwaunza, L., Terera, G., Mahachi, C., Murambiwa, P., Machiweni, T. and Mapanga, R. (2017). Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. The Lancet. http://dx.doi.org/10.1016/S0140-6736(17)32252-3 |
The Awareness domain contains research, news, information, observations, and ideas at the level of self in an effort to intellectualize health concepts.
The Lifestyle domain builds off intellectual concepts and offers practical applications.
Taking care of yourself is at the core of the other domains because the others depend on your health and wellness.
Archives
May 2024
Categories
All
|


 RSS Feed
RSS Feed





