
|
Hydrogen comes in two “flavors”: regular hydrogen, which is actually called protium, and deuterium. Deuterium has all of the same properties as hydrogen, except that it's twice as big and heavy. This is due to an added neutron paired with the proton in the nucleus. Because of this, deuterium is also referred to as "heavy hydrogen," and it actually behaves quite differently from regular hydrogen in chemical reactions and in our bodies. In nature, deuterium helps things grow. For example, deuterium is biologically necessary for growth in babies, teenagers, and developing plants and animals. But once you stop growing, having too much deuterium in your cells can result in mitochondrial dysfunction and lead to premature aging, metabolic problems, and disease. 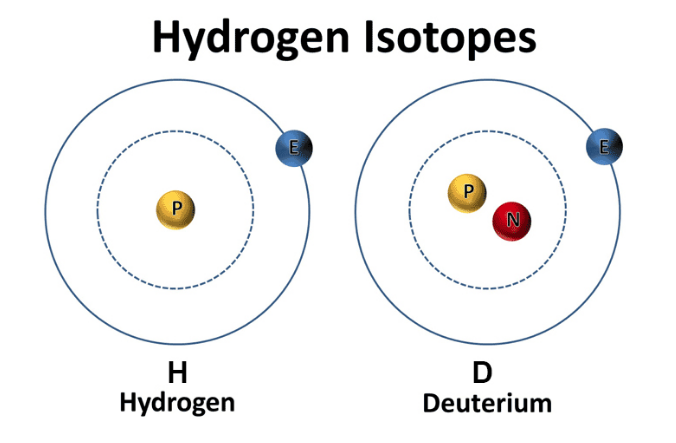 Image from ddcenters.com Deuterium is like thick, gluggy oil - when you put thick oil into an engine, the engine sputters, makes strange noises, and eventually breaks. Nature has put systems in place to deplete deuterium and protect the nanomotors, or "little engines," in our cells’ mitochondria from coming into contact with this thick oil. However, the side effects of a modern life - pollution, global warming, processed foods, less healthy lifestyles, etc. - have resulted in many people having way too much deuterium inside their cells. This results in an inability to effectively deplete deuterium and the destruction of our nanomotors. This starts a vicious cycle of deuterium building up and breaking more of our nanomotors. Fewer nanomotors means less energy and more sickness and disease. While deuterium is a natural and essential element, its presence has increased in the modernized environment within the food, atmosphere, and water. Deuterium levels is food will vary based o where that food is grown - deuterium is highest in the equator and in low elevations. Foods high in fat, as well as green plants, including algae and spirulina, which contain high amounts of chlorophyll, are lower in deuterium than fruits, roots, and underground vegetables. As it turns out, GMO foods tainted with glyphosate, as well as processed, synthetically made foods, possess high amounts of deuterium. There are various lifestyle practices that have led to increased deuterium levels including a lack of sleep, particularly deep REM sleep. In addition, breathing shallow and fast via the mouth and chest also contributes to elevated levels of deuterium. Researchers have demonstrated that elevated of deuterium can contribute to:
Learn More About Deuterium Depletion References Understanding Deuterium - The Center for Deuterium Depletion. (2019). Retrieved 24 December 2019, from https://www.ddcenters.com/about-deuterium-2-2-2/
2 Comments
It's that time: time to test your blood. Most blood tests include a fasting lipid panel to assess one's risk of cardiovascular disease. A lipid panel is a test that measures fats and fatty substances used as a source of energy in the body. Lipids include cholesterol, triglycerides, high-density lipoprotein (HDL) and low-density lipoprotein (LDL). What Are Triglycerides?
Triglycerides are a powerful cardiovascular risk marker. Elevated triglyceride levels are a hallmark of too many carbohydrates in the diet. 60 percent of fructose is shunted toward the liver, where it is converted to triglycerides (which causes heart disease) (Gundry, 2017). In fact, fructose, which is the sugar found in most processed foods (often in the form of high-fructose corn syrup) can only be metabolized by your liver. If you eat a typical Western-style diet, you consume high amounts of it. The overload of fructose ends up damaging your liver in the same way alcohol and other toxins do (Mercola, 2017). 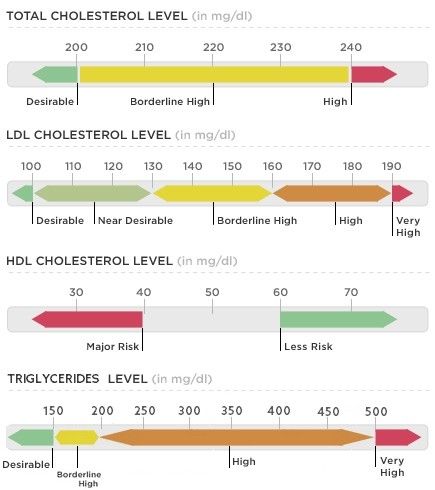 What about Cholesterol? Our culture is obsessed with cholesterol levels, to the point that one in four adults in the U.S. take a statin drug to lower cholesterol levels. Nevertheless, elevated cholesterol levels are rarely a risk factor for heart disease, although elevated triglycerides clearly are. Fortunately, elevated triglycerides can easily be corrected and lowered to an ideal level of below 75 with the proper lifestyle interventions. The following tests can give you a far better assessment of your heart disease risk than your total cholesterol alone:
Influence of Triglycerides on Leptin High triglyceride levels (over 100 mg/dL) is known to cause leptin resistance. Leptin is a hormone located in fat cells, and like most hormones, it's function is complex. Leptin is tied to the coordination of our metabolic, hormonal, and behavioral response to starvation. Leptin essentially controls mammalian metabolism. Leptin decides whether to make us hungry and store more fat or burn fat. In other words, when your stomach is full, fat cells release leptin to tell your brain to stop eating. This is why people with low levels of leptin are prone to overeating. One study observed participants with a 20 percent drop in leptin experienced a 24 percent increase in hunger and appetite, influencing their cravings for calorie-dense, high-carbohydrate foods, especially sweets, salty snacks, and starchy foods. The researchers discovered the drop in leptin was caused by sleep deprivation. Leptin is also a pro-inflammatory molecule - it controls the creation of other inflammatory moleciles in your fat tissue throughout your body. This explains why overweight individuals are susceptible to inflammatory problems. Leptin is ranked highly on the body's chain of command, so imbalances tend to spiral downward and wreak havoc on virtually every system of the body beyond those directly controlled by leptin. Leptin, like insulin, is negatively influenced by carbohydrates. The more refined and processed the carbohydrate, the more imbalanced leptin levels become. When the body is overloaded and overwhelmed by substances that cause continuous surges in leptin, leptin receptors begin to turn off and you become leptin resistant. So even though leptin is now elevated, it doesn't work - it won't signal to your brain that you're full so you can stop eating. Not a single drug or supplement can balance leptin levels. But better sleep, as well as better dietary choices will (Perlmutter, 2013). Causes of High Triglycerides
The main culprit Preventing cardiovascular disease involves reducing chronic inflammation in your body, and a proper diet is an absolute cornerstone. Although saturated fat has taken the blame for causing heart disease for the last several decades, the primary culprit in heart disease is sugar consumption. A 2015 study published in the Journal of the American Medical Association concluded that there is " a significant relationship between added sugar consumption and increased risk for cardiovascular mortality." the 15-year study, which included data for 31,000 Americans, found that those who consumed 25 percent or more of their daily calories as added sugars were more than twice as likely to die form heart disease as those who got less than 10 percent of their calories from sugar. On the whole, the odds of dying from heart disease rose in tandem with the percentage of added sugar in the diet regardless of the age, sex, physical activity level, and body mass index (Dhurandhar & Thomas, 2014). A 2014 study came to very similar conclusions. Here, those who consumed the most sugar - about 25 percent of their daily calories - were twice as likely to die form heart disease as those who limited their sugar intake to 7 percent of their total calories (Yang et al., 2013). A 2013 study, published in the Journal of the Academy of Nutrition and Dietetics, looked at the differing effects of high-fat diets versus low-fat diets on blood lipid levels. The study included 32 studies and found that high-fat diets resulted in significantly greater improvements in reductions of total cholesterol, LDL cholesterol, and triglycerides and benificial increases in HDL cholesterol (Schwingshackl et al., 2013). How to Lower Triglycerides
Consider a Detox
The Dangers of StatinsSo, why are we all obsessed with total cholesterol and LDL cholesterol when we know they aren’t the primary culprits for heart attacks? Because a multi-billion dollar drug industry exists behind the number-one best-selling class of drugs on the market: Statins. Of course, the choice to take medications, if referred by your physician is, and should, always be your choice. However, you have the right to be fully informed of the side effects of consuming anything. With this in mind, it is important to be aware of the unintended side effects of taking statins. A study published in Clinical Cardiology concluded that "Statin therapy is associated with decreased myocardial [heart muscle] function," which often leads to heart failure. The study did not address causes, but it's widely known that statins lower your CoQ10 levels by blocking the pathway involved in cholesterol production -- the same pathway by which Q10 is produced. Statins also reduce the blood cholesterol that transports CoQ10 and other fat-soluble antioxidants. The loss of CoQ10 leads to loss of cell energy and increased free radicals which, in turn, can further damage your mitochondrial DNA, effectively setting into motion an evil circle of increasing free radicals and mitochondrial damage (Mercola, 2011). Moreover, for those at risk of heart disease taking statins who are unwilling or unable to bring down their cholesterol and/or triglyceride levels naturally with dietary changes, the potential for liver or muscle damage should be acknowledged. In addition, the potential for brain-related side effects, such as memory loss and confusion, as well as Parkinson’s-like symptoms is of concern. Statin drugs also appeared to increase the risk of stroke and developing diabetes. In 2013, a study of several thousand breast cancer patients reported that long-term use of statins may as much as double a woman's risk of invasive breast cancer. There are 71 diseases that may be associated with these drugs, and this is only the tip of the iceberg. There are actually over 900 studies showing the risks of statin drugs, which include:
Plant-based diets have been shown to lower cholesterol just as effectively as first-line statin drugs, but without the risks. In fact, the "side effects" of healthy eating tend to be good - less cancer and diabetes risks and protection of the liver and brain (Gregor, 2015). What Should you Eat? 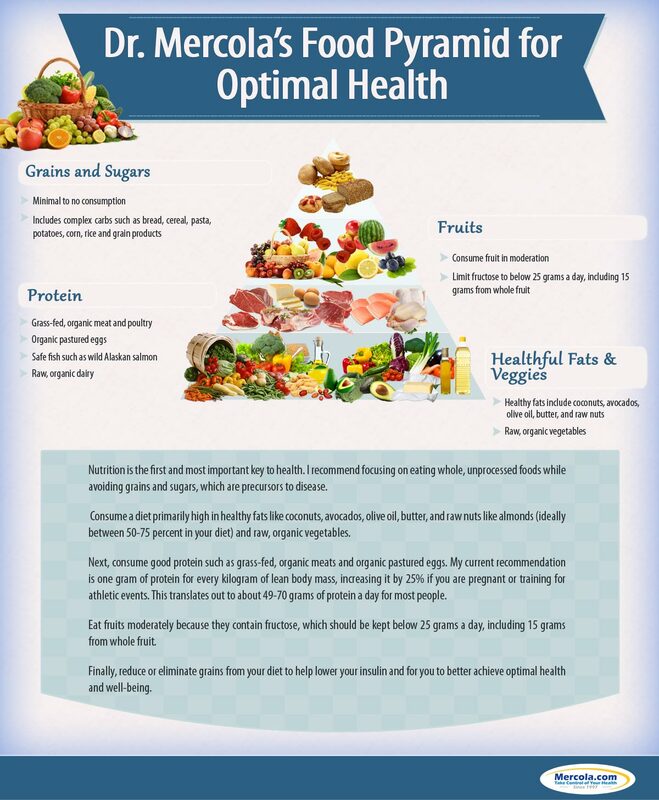 ReferencesBaker, A. (2012). What's the real driver of elevated cholesterol? hint: it's not saturated fat! - Nourish Holistic Nutrition. [online] Nourish Holistic Nutrition. Available at: nourishholisticnutrition.com/whats-the-real-driver-of-elevated-cholesterol/ [Accessed 8 Feb. 2019].
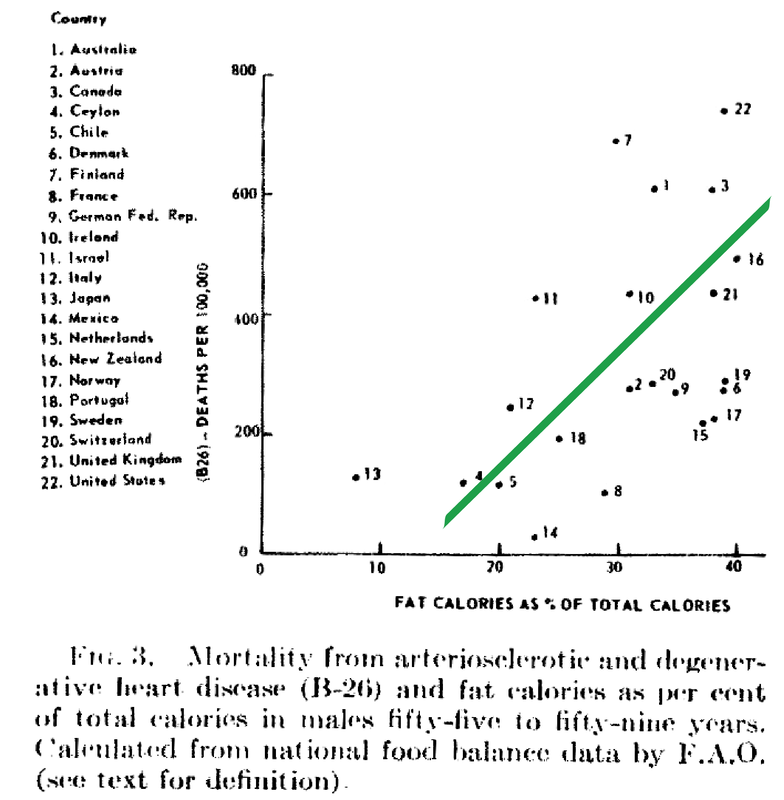
Dhurandhar, N. and Thomas, D. (2015). The Link Between Dietary Sugar Intake and Cardiovascular Disease Mortality. JAMA, 313(9), p.959. https://doi.org/10.1001/jama.2014.18267 [Accessed 8 Feb. 2019]. Gregor, M. (2015) How Not to Die. London: Pan Books Gundry, S. (2017). The Plant Paradox. New York, NY: Harper Wave Hyman, M. (2016). 7 Ways to Optimize Cholesterol. [online] Dr. Mark Hyman. Available at: https://drhyman.com/blog/2016/01/14/7-ways-to-optimize-cholesterol/ [Accessed 8 Feb. 2019]. Mercola, J. (2017). Fat for Fuel. Carlsbad, CA: Hayhouse Inc. Mercola, J. (2011). New Study Shows Using Statins Actually Harms Heart Function. [online] Mercola.com. Available at: https://articles.mercola.com/sites/articles/archive/2011/06/22/new-study-show-using-statins-actually-worsens-your-heart-function.aspx [Accessed 8 Feb. 2019]. Mercola, J. (2015). Conventional Heart Disease Advice May Make Matters Worse. [online] Mercola.com. Available at: https://articles.mercola.com/sites/articles/archive/2015/08/02/heart-disease-risk-factors.aspx [Accessed 8 Feb. 2019]. Perlmutter, D (2013). Grain Brain. New York, NY: Little Brown Ray, K. et al. (2010). Statins and All-Cause Mortality in High-Risk Primary Prevention. Archives of Internal Medicine, 170(12), p.1024. Available at: https://doi.org/10.1001/archinternmed.2010.182 [Accessed 8 Feb. 2019]. Rubinstein, J., Aloka, F. and Abela, G. (2009). Statin Therapy Decreases Myocardial Function as Evaluated Via Strain Imaging. Clinical Cardiology, 32(12), pp.684-689. Available at: https://doi.org/10.1002/clc.20644 [Accessed 8 Feb. 2019]. Schwingshackl, S., et al. (2013). Comparison of Effects of Long-Term Low-Fat vs High-Fat Diets on Blood Lipid Levels in Overweight and Obese Patients: A Systematic Review and Meta-Analysis. Journal of the Academy of Nutrition and Dietetics, 113(12), pp. 1640-61. Available at: https://doi.org/10.1016/j.jand.2013.07.010 [Accessed 8 Feb. 2019]. Wallerwellness.com. (2019). Understanding Triglycerides. [online] Available at: https://www.wallerwellness.com/health-and-aging/understanding-triglycerides [Accessed 8 Feb. 2019]. Williams, J. (2017). How To Lower Dangerously High Triglyceride Levels. [online] Renegade Health. Available at: http://renegadehealth.com/blog/2017/03/31/how-to-lower-dangerously-high-triglycerides-levels [Accessed 8 Feb. 2019]. Yang, Q., et al. (2014). Added Sugar Intake and Cardiovascular Diseases Mortality Among US Adults. JAMA Internal Medicine, 174(4), pp.516-24. Available at: https://doi.org/10.1001/jamainternmed.2013.13563 [Accessed 8 Feb. 2019]. Despite food manufacturers claiming that refined vegetable oils were healthy, Americans experienced an up-rise in heart disease during the early 20th century. Like many new inventions, few questions were initially posited. Unfortunately, an alternate nutrient took the blame due to the research of a single scientist. In 1951, American physiologist and professor Ancel Keys went to Europe in search of the cause of cardiovascular disease. In his quest, he went to observe the eating habits of individuals living Naples, Italy due to reports of a low prevalence of heart disease. During this time, post-war conditions resulted in finite and unusual circumstances in regards to agriculture and infrastructure. Therefore what Keys perceived as a cultural tradition was dubbed the "Mediterranean diet". Keys observed the residents in Naples consumed primarily pasta and plain pizza, with vegetables, olive oil, cheese, fruit for dessert, a moderate amount of wine, and very little meat (except among individuals belonging to a higher socioeconomic status).  Through an informal study measuring cholesterol serum levels among Rotary club members (those who could not afford meat, but could afford cheese) conducted by Keys's wife, whom at the time was a medical technologist, Keys deduced that avoiding meat resulted in a lower incidence of heart attacks. Ancel Keys continued on his biased search for proof that a diet high in saturated fat is correlated with a higher risk of cardiovascular disease. He eventually compiled data from six more countries with high rates of heart disease and diets typically high in saturated fat. At first glance, Keys's research seemed logical and compelling. The evidence was based on the premise that individuals in America, who consumed high amounts of saturated fat, died from heart disease at a higher rate than individuals in Japan, who consumed low amounts of saturated fat.
Unfortunately, Keys had gained the interest of people in positions of power. Upon President Eisenhower's heart attack in 1955, Keys proposed his theory to the president's primary care physician, Paul Dudley White. Days following, White began to advise to the public to reduce the consumption of saturated fat and cholesterol in an effort to prevent cardiovascular disease. Through his connections and influence, Keys soon joined the nutrition committee of the American Heart Association (AHA) which, based on Keys's research, released a report in 1961 that advised patients with a high risk of cardiovascular disease to reduce their consumption of saturated fat. (Interestingly enough, the AHA began its rise to prominence in 1948, the same year Proctor & Gamble donated over $1.7 million to the organization - resulting in the AHA indebted to Crisco.) In 1961, Time magazine placed Ancel Keys on the front cover touting him as "the twenthiest century's most influential nutrition expert." By 1970, Keys published the Seven Countries Study, which detailed his original research - this study has now been cited in over a million other scientific publications. While Keys associative observations between saturated fat and cardiovascular disease never proved causation, he had won the battle of public opinion. With the help of Ancel Keys, the American medical community and mainstream media has advised consumers to stop eating the animal products that have been consumed for centuries, replacing them with bread, pasta, margarine, low-fat dairy, and vegetable oil. This was the dietary shift that was codified by the United States government in the late 1970s. References Central Committee for Medical And Community Program of the American Heart Association. (1961). Dietary Fat and Its Relation to Heart Attacks and Strokes. Circulation [online] 23, pp.133-36. Available at: https://circ.ahajournals.org/content/circulationaha/23/1/133.full.pdf [Accessed 26 Jan. 2019]
Keys, A. (1953). Atherosclerosis: A Problem in Newer Public Health. Journal of Mt. Sinai Hospital, [online] 20(2), pp.118-39. Keys, A. (1970). Coronary Heart Disease in Seven Countries. Circulation. 41 (1), pp.1186-95. Keys, A. (1995). Mediterranean Diet and Public Health: Personal Reflections. American Journal of Clinical Nutrition, [online] 61 (6), pp.1321S-1323S. Available at: https://dx.doi.org/10.1093/ajcn/61.6.1321s [Accessed 26 Jan. 2019] Marvin, H. (1964). The 40 Year War on Heart Disease. New York: American Heart Association. Mercola, J. (2017). Fat For Fuel. Carlsbad, California: Hay House. Teichholz, N. (2014). The Big Fat Surprise. New York: Simon & Schuster, pp.32-33.
Physiologically, fasting:
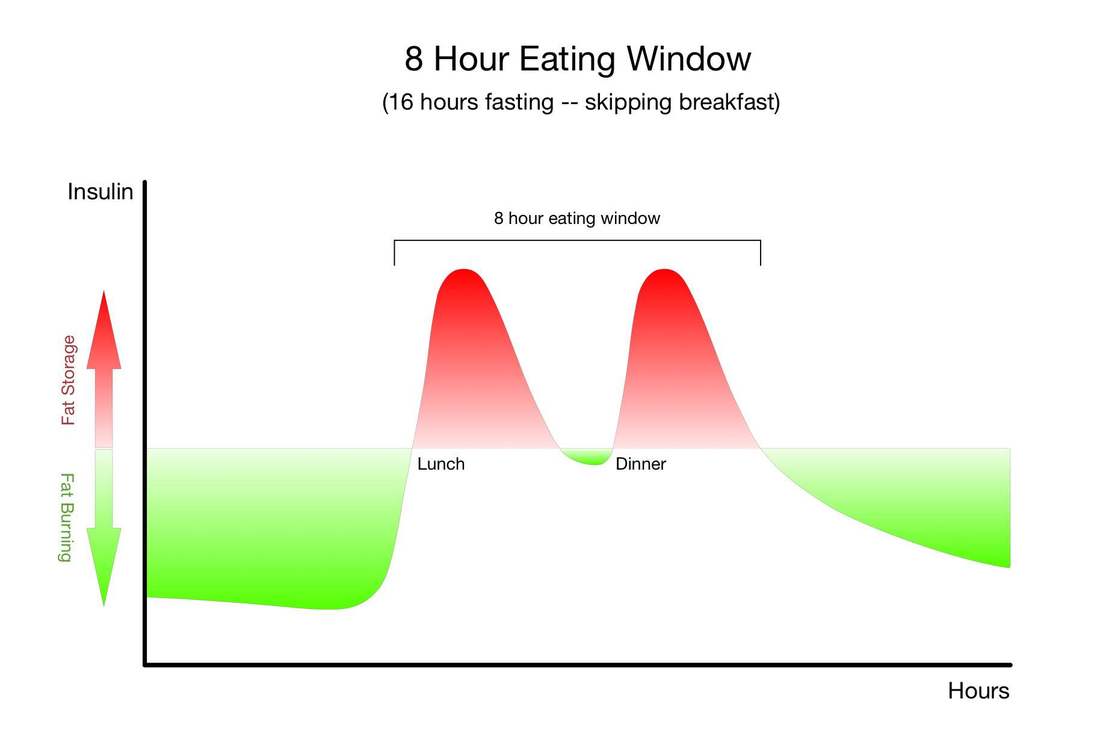
The only other strategy that has so many research-baked benefits for longevity is long-term calorie restriction, which requires a significant long-term reduction in the amount of food you eat so that you are essentially living on the brink of starvation. Compliance with calorie-restricted diets is abysmal. Fortunately, there are many ways to fast, and there is likely a form of fasting out there that you will be able to tolerate and incorporate into your life. It's important for you to remember that fasting can provide nearly identical benefits without the pain, suffering, and compliance challenges of calorie restriction. Instead of regulating how much food you eat, as with long-term calorie restriction, you only need to modify when you eat - and of course wisely choose the foods you do eat.Simply cycling between periods of eating and fasting on a daily, weekly, or monthly schedule has been shown to provide many of the same benefits as long-term calorie restriction. Choosing when to eat and when to fast in this way is known as "intermittent fasting." "Don't eat less - eat less often." |

| It is well established that diet is one of the most important modifiable risk factors for cardiovascular disease and other non-transmittable diseases. Current dietary guidelines recommend a low-fat diet (<30% of energy) and limiting saturated fatty acids to less than 10% of energy intake by replacing them with unsaturated fatty acids, while consuming 45-65% of of total calories from carbohydrates. However, results from an international study, spanning more than a decade, are prompting experts to reconsider global dietary guidelines. |  Image from Well-being Secrets |
The Prospective Urban Rural Epidemiology (PURE) study is a large, epidemiological study that included more than 135,000 individuals between the ages of 35–70 years across 18 countries. Regions included Canada, Sweden, United Arab Emirates, Argentina, Brazil, Chile, China, Colombia, Iran, Malaysia, occupied Palestinian territory, Poland, South Africa, Turkey, Bangladesh, India, Pakistan, and Zimbabwe.
Overall, the researchers found that high carbohydrate intake (more than 60% of energy) was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke.
For decades, dietary guidelines have focused on reducing total fat and saturated fatty acid intake, based on the presumption that replacing saturated fatty acids with carbohydrate and unsaturated fats will lower LDL cholesterol and should therefore reduce cardiovascular disease events. This focus is largely based on selective emphasis on some observational and clinical data, despite the existence of several randomized trials and observational studies that do not support these conclusions.
Overall, the researchers found that high carbohydrate intake (more than 60% of energy) was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke.
For decades, dietary guidelines have focused on reducing total fat and saturated fatty acid intake, based on the presumption that replacing saturated fatty acids with carbohydrate and unsaturated fats will lower LDL cholesterol and should therefore reduce cardiovascular disease events. This focus is largely based on selective emphasis on some observational and clinical data, despite the existence of several randomized trials and observational studies that do not support these conclusions.
Results of the Study
After documenting 5796 deaths and 4784 major cardiovascular disease events and running statistical analyses, the researchers observed:
- Individuals who consumed a very high carbohydrate diet (at least 60% of energy), especially from refined sources (such as white rice and white bread), were associated with increased risk of total mortality and cardiovascular events.
- An inverse association between total fat and total mortality.
- Individuals consuming a higher glycemic load, such as refined carbohydrates, were associated with a higher risk of stroke
- An inverse association between saturated fatty acid intake, total mortality, non-
cardiovascular disease mortality, and stroke risk without any evidence of an increase in major cardiovascular disease, myocardial infarction, and cardiovascular disease mortality. - An inverse association between monounsaturated fatty acid intake and total mortality.
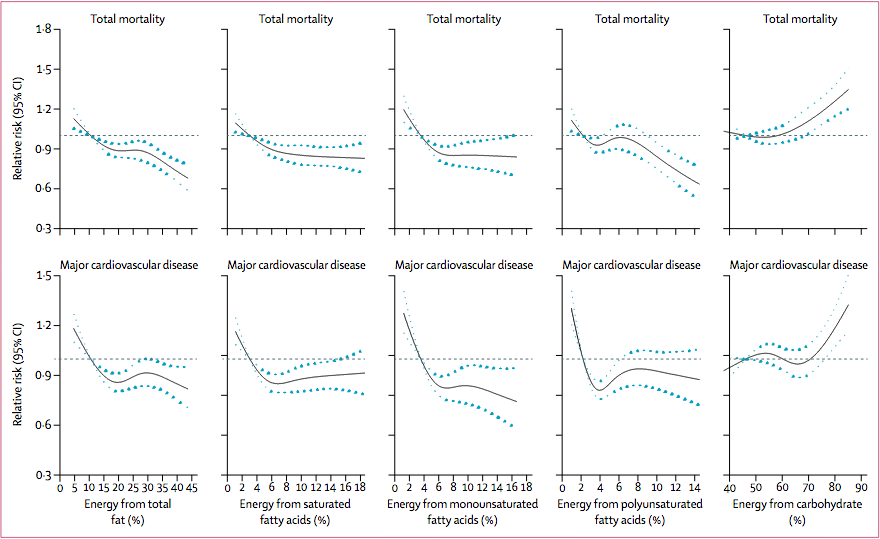
Association between estimated percentage energy from nutrients and total mortality and major cardiovascular disease (n=135335). Image from (Dehghan et al., 2017)
Recommendations and Take Away
The results of this study do not suggest a low-carbohydrate diet, but rather that a total fat intake of about 35% of energy while lowering carbohydrate intake might lower risk of total mortality. Collectively, the data does not support the recommendation to limit saturated fatty acids to less than 10% of intake and that a very low intake (ie, below about 7% of energy) might even be harmful.
Limitations of the Study
- The researchers used food frequency questionnaires (FFQs) to estimate participants’ dietary intake which is not a measure of absolute intake, but is suited for classifying individuals into intake categories and is the most commonly used approach for assessing intake in epidemiological studies.
- Dietary intakes were measured only at baseline, and it is possible that dietary changes might have occurred during the follow-up period. Even if major dietary changes occurred after the baseline assessment, they probably would have weakened the observed associations.
- There is potential for social desirability bias and individuals who are health conscious might also adopt other healthy lifestyles. However, if this were the case, the researchers would not expect to see different associations for the different outcomes.
- As with any observational cohort study, observed associations might be in part due to residual confounding (eg, differences in the ability to afford fats and animal proteins, which are more expensive than carbohydrates) despite extensive adjustment for known confounding factors.
- The researchers were unable to measure trans-fat intake which might affect our results, especially our replacement analyses.
- FFQ assessed polyunsaturated fatty acid intake mainly from foods, rather than from vegetable oils, which might have different health effects than those observed in the study.
The researchers declare no conflicts of interests
References
Brown, E. (2017). More Evidence That Everything the Government Teaches Us About Eating Is Wrong. [online] Reason.com. Available at: http://reason.com/blog/2017/08/30/pure-study-challenges-dietary-dogma [Accessed 20 Sep. 2017].
Dehghan, M., Mente, A., Zhang, X., Swaminathan, S., Li, W., Mohan, V., Iqbal, R., Kumar, R., Wentzel-Viljoen, E., Rosengren, A., Amma, L., Avezum, A., Chifamba, J., Diaz, R., Khatib, R., Lear, S., Lopez-Jaramillo, P., Liu, X., Gupta, R., Mohammadifard, N., Gao, N., Oguz, A., Ramli, A., Seron, P., Sun, Y., Szuba, A., Tsolekile, L., Wielgosz, A., Yusuf, R., Hussein Yusufali, A., Teo, K., Rangarajan, S., Dagenais, G., Bangdiwala, S., Islam, S., Anand, S., Yusuf, S., Diaz, R., Orlandini, A., Linetsky, B., Toscanelli, S., Casaccia, G., Cuneo, J., Rahman, O., Yusuf, R., Azad, A., Rabbani, K., Cherry, H., Mannan, A., Hassan, I., Talukdar, A., Tooheen, R., Khan, M., Sintaha, M., Choudhury, T., Haque, R., Parvin, S., Avezum, A., Oliveira, G., Marcilio, C., Mattos, A., Teo, K., Yusuf, S., Dejesus, J., Agapay, D., Tongana, T., Solano, R., Kay, I., Trottier, S., Rimac, J., Elsheikh, W., Heldman, L., Ramezani, E., Dagenais, G., Poirier, P., Turbide, G., Auger, D., De Bluts, A., Proulx, M., Cayer, M., Bonneville, N., Lear, S., Gasevic, D., Corber, E., de Jong, V., Vukmirovich, I., Wielgosz, A., Fodor, G., Pipe, A., Shane, A., Lanas, F., Seron, P., Martinez, S., Valdebenito, A., Oliveros, M., Wei, L., Lisheng, L., Chunming, C., Xingyu, W., Wenhua, Z., Hongye, Z., Xuan, J., Bo, H., Yi, S., Jian, B., Xiuwen, Z., Xiaohong, C., Tao, C., Hui, C., Xiaohong, C., Qing, D., Xiaoru, C., Qing, D., Xinye, H., Bo, H., Xuan, J., Jian, L., Juan, L., Xu, L., Bing, R., Yi, S., Wei, W., Yang, W., Jun, Y., Yi, Z., Hongye, Z., Xiuwen, Z., Manlu, Z., Fanghong, L., Jianfang, W., Yindong, L., Yan, H., Liangqing, Z., Baoxia, G., Xiaoyang, L., Shiying, Z., Rongwen, B., Xiuzhen, T., Dong, L., Di, C., Jianguo, W., Yize, X., Tianlu, L., Peng, Z., Changlin, D., Ning, L., Xiaolan, M., Yuqing, Y., Rensheng, L., Minfan, F., Jing, H., Yu, L., Xiaojie, X., Qiang, Z., Lopez-Jaramillo, P., Lopez, P., Garcia, R., Jurado, L., Gómez-Arbeláez, D., Arguello, J., Dueñas, R., Silva, S., Pradilla, L., Ramirez, F., Molina, D., Cure-Cure, C., Perez, M., Hernandez, E., Arcos, E., Fernandez, S., Narvaez, C., Paez, J., Sotomayor, A., Garcia, H., Sanchez, G., David, T., Rico, A., Mony, P., Vaz, M., Bharathi, A., Swaminathan, S., Kurpad, K., Jayachitra, K., Kumar, N., Hospital, H., Mohan, V., Deepa, M., Parthiban, K., Anitha, M., Hemavathy, S., Rahulashankiruthiyayan, T., Anitha, D., Sridevi, K., Gupta, R., Panwar, R., Mohan, I., Rastogi, P., Rastogi, S., Bhargava, R., Kumar, R., Thakur, J., Patro, B., Lakshmi, P., Mahajan, R., Chaudary, P., Kutty, V., Vijayakumar, K., Ajayan, K., Rajasree, G., Renjini, A., Deepu, A., Sandhya, B., Asha, S., Soumya, H., Kelishadi, R., Bahonar, A., Mohammadifard, N., Heidari, H., Yusoff, K., Ismail, T., Ng, K., Devi, A., Nasir, N., Yasin, M., Miskan, M., Rahman, E., Arsad, M., Ariffin, F., Razak, S., Majid, F., Bakar, N., Yacob, M., Zainon, N., Salleh, R., Ramli, M., Halim, N., Norlizan, S., Ghazali, N., Arshad, M., Razali, R., Ali, S., Othman, H., Hafar, C., Pit, A., Danuri, N., Basir, F., Zahari, S., Abdullah, H., Arippin, M., Zakaria, N., Noorhassim, I., Hasni, M., Azmi, M., Zaleha, M., Hazdi, K., Rizam, A., Sazman, W., Azman, A., Khatib, R., Khammash, U., Khatib, A., Giacaman, R., Iqbal, R., Afridi, A., Khawaja, R., Raza, A., Kazmi, K., Zatonski, W., Szuba, A., Zatonska, K., Ilow, R., Ferus, M., Regulska-Ilow, B., Rózanska, D., Wolyniec, M., Alkamel, Ali, M., Kruger, M., Voster, H., Schutte, A., Wentzel-Viljoen, E., Eloff, F., de Ridder, H., Moss, H., Potgieter, J., Roux, A., Watson, M., de Wet, G., Olckers, A., Jerling, J., Pieters, M., Hoekstra, T., Puoane, T., Igumbor, E., Tsolekile, L., Sanders, D., Naidoo, P., Steyn, N., Peer, N., Mayosi, B., Rayner, B., Lambert, V., Levitt, N., Kolbe-Alexander, T., Ntyintyane, L., Hughes, G., Swart, R., Fourie, J., Muzigaba, M., Xapa, S., Gobile, N., Ndayi, K., Jwili, B., Ndibaza, K., Egbujie, B., Rosengren, A., Boström, K., Gustavsson, A., Andreasson, M., Snällman, M., Wirdemann, L., Oguz, A., Imeryuz, N., Altuntas, Y., Gulec, S., Temizhan, A., Karsidag, K., Calik, K., Akalin, A., Caklili, O., Keskinler, M., Erbakan, A., Yusufali, A., Almahmeed, W., Swidan, H., Darwish, E., Hashemi, A., Al-Khaja, N., Muscat-Baron, J., Ahmed, S., Mamdouh, T., Darwish, W., Abdelmotagali, M., Awed, S., Movahedi, G., Hussain, F., Al Shaibani, H., Gharabou, R., Youssef, D., Nawati, A., Salah, Z., Abdalla, R., Al Shuwaihi, S., Al Omairi, M., Cadigal, O., Alejandrino, R., Chifamba, J., Gwaunza, L., Terera, G., Mahachi, C., Murambiwa, P., Machiweni, T. and Mapanga, R. (2017). Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. The Lancet. http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Dehghan, M., Mente, A., Zhang, X., Swaminathan, S., Li, W., Mohan, V., Iqbal, R., Kumar, R., Wentzel-Viljoen, E., Rosengren, A., Amma, L., Avezum, A., Chifamba, J., Diaz, R., Khatib, R., Lear, S., Lopez-Jaramillo, P., Liu, X., Gupta, R., Mohammadifard, N., Gao, N., Oguz, A., Ramli, A., Seron, P., Sun, Y., Szuba, A., Tsolekile, L., Wielgosz, A., Yusuf, R., Hussein Yusufali, A., Teo, K., Rangarajan, S., Dagenais, G., Bangdiwala, S., Islam, S., Anand, S., Yusuf, S., Diaz, R., Orlandini, A., Linetsky, B., Toscanelli, S., Casaccia, G., Cuneo, J., Rahman, O., Yusuf, R., Azad, A., Rabbani, K., Cherry, H., Mannan, A., Hassan, I., Talukdar, A., Tooheen, R., Khan, M., Sintaha, M., Choudhury, T., Haque, R., Parvin, S., Avezum, A., Oliveira, G., Marcilio, C., Mattos, A., Teo, K., Yusuf, S., Dejesus, J., Agapay, D., Tongana, T., Solano, R., Kay, I., Trottier, S., Rimac, J., Elsheikh, W., Heldman, L., Ramezani, E., Dagenais, G., Poirier, P., Turbide, G., Auger, D., De Bluts, A., Proulx, M., Cayer, M., Bonneville, N., Lear, S., Gasevic, D., Corber, E., de Jong, V., Vukmirovich, I., Wielgosz, A., Fodor, G., Pipe, A., Shane, A., Lanas, F., Seron, P., Martinez, S., Valdebenito, A., Oliveros, M., Wei, L., Lisheng, L., Chunming, C., Xingyu, W., Wenhua, Z., Hongye, Z., Xuan, J., Bo, H., Yi, S., Jian, B., Xiuwen, Z., Xiaohong, C., Tao, C., Hui, C., Xiaohong, C., Qing, D., Xiaoru, C., Qing, D., Xinye, H., Bo, H., Xuan, J., Jian, L., Juan, L., Xu, L., Bing, R., Yi, S., Wei, W., Yang, W., Jun, Y., Yi, Z., Hongye, Z., Xiuwen, Z., Manlu, Z., Fanghong, L., Jianfang, W., Yindong, L., Yan, H., Liangqing, Z., Baoxia, G., Xiaoyang, L., Shiying, Z., Rongwen, B., Xiuzhen, T., Dong, L., Di, C., Jianguo, W., Yize, X., Tianlu, L., Peng, Z., Changlin, D., Ning, L., Xiaolan, M., Yuqing, Y., Rensheng, L., Minfan, F., Jing, H., Yu, L., Xiaojie, X., Qiang, Z., Lopez-Jaramillo, P., Lopez, P., Garcia, R., Jurado, L., Gómez-Arbeláez, D., Arguello, J., Dueñas, R., Silva, S., Pradilla, L., Ramirez, F., Molina, D., Cure-Cure, C., Perez, M., Hernandez, E., Arcos, E., Fernandez, S., Narvaez, C., Paez, J., Sotomayor, A., Garcia, H., Sanchez, G., David, T., Rico, A., Mony, P., Vaz, M., Bharathi, A., Swaminathan, S., Kurpad, K., Jayachitra, K., Kumar, N., Hospital, H., Mohan, V., Deepa, M., Parthiban, K., Anitha, M., Hemavathy, S., Rahulashankiruthiyayan, T., Anitha, D., Sridevi, K., Gupta, R., Panwar, R., Mohan, I., Rastogi, P., Rastogi, S., Bhargava, R., Kumar, R., Thakur, J., Patro, B., Lakshmi, P., Mahajan, R., Chaudary, P., Kutty, V., Vijayakumar, K., Ajayan, K., Rajasree, G., Renjini, A., Deepu, A., Sandhya, B., Asha, S., Soumya, H., Kelishadi, R., Bahonar, A., Mohammadifard, N., Heidari, H., Yusoff, K., Ismail, T., Ng, K., Devi, A., Nasir, N., Yasin, M., Miskan, M., Rahman, E., Arsad, M., Ariffin, F., Razak, S., Majid, F., Bakar, N., Yacob, M., Zainon, N., Salleh, R., Ramli, M., Halim, N., Norlizan, S., Ghazali, N., Arshad, M., Razali, R., Ali, S., Othman, H., Hafar, C., Pit, A., Danuri, N., Basir, F., Zahari, S., Abdullah, H., Arippin, M., Zakaria, N., Noorhassim, I., Hasni, M., Azmi, M., Zaleha, M., Hazdi, K., Rizam, A., Sazman, W., Azman, A., Khatib, R., Khammash, U., Khatib, A., Giacaman, R., Iqbal, R., Afridi, A., Khawaja, R., Raza, A., Kazmi, K., Zatonski, W., Szuba, A., Zatonska, K., Ilow, R., Ferus, M., Regulska-Ilow, B., Rózanska, D., Wolyniec, M., Alkamel, Ali, M., Kruger, M., Voster, H., Schutte, A., Wentzel-Viljoen, E., Eloff, F., de Ridder, H., Moss, H., Potgieter, J., Roux, A., Watson, M., de Wet, G., Olckers, A., Jerling, J., Pieters, M., Hoekstra, T., Puoane, T., Igumbor, E., Tsolekile, L., Sanders, D., Naidoo, P., Steyn, N., Peer, N., Mayosi, B., Rayner, B., Lambert, V., Levitt, N., Kolbe-Alexander, T., Ntyintyane, L., Hughes, G., Swart, R., Fourie, J., Muzigaba, M., Xapa, S., Gobile, N., Ndayi, K., Jwili, B., Ndibaza, K., Egbujie, B., Rosengren, A., Boström, K., Gustavsson, A., Andreasson, M., Snällman, M., Wirdemann, L., Oguz, A., Imeryuz, N., Altuntas, Y., Gulec, S., Temizhan, A., Karsidag, K., Calik, K., Akalin, A., Caklili, O., Keskinler, M., Erbakan, A., Yusufali, A., Almahmeed, W., Swidan, H., Darwish, E., Hashemi, A., Al-Khaja, N., Muscat-Baron, J., Ahmed, S., Mamdouh, T., Darwish, W., Abdelmotagali, M., Awed, S., Movahedi, G., Hussain, F., Al Shaibani, H., Gharabou, R., Youssef, D., Nawati, A., Salah, Z., Abdalla, R., Al Shuwaihi, S., Al Omairi, M., Cadigal, O., Alejandrino, R., Chifamba, J., Gwaunza, L., Terera, G., Mahachi, C., Murambiwa, P., Machiweni, T. and Mapanga, R. (2017). Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. The Lancet. http://dx.doi.org/10.1016/S0140-6736(17)32252-3
The Awareness domain contains research, news, information, observations, and ideas at the level of self in an effort to intellectualize health concepts.
The Lifestyle domain builds off intellectual concepts and offers practical applications.
Taking care of yourself is at the core of the other domains because the others depend on your health and wellness.
Archives
May 2024
April 2024
March 2024
February 2024
January 2024
December 2023
September 2023
August 2023
June 2023
October 2022
July 2022
February 2022
January 2022
December 2021
November 2021
October 2021
August 2021
July 2021
June 2021
March 2021
February 2021
January 2021
December 2020
November 2020
September 2020
August 2020
March 2020
December 2019
November 2019
October 2019
September 2019
August 2019
July 2019
May 2019
April 2019
March 2019
February 2019
January 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
April 2018
March 2018
February 2018
January 2018
December 2017
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017
Categories
All
5G
Adductors
Anxiety
Autism
Ayurveda
Big Pharma
Body
Breathing
Cancer
Cannabis
Carbohydrates
Cardiovascular Disease
Children
Chronic Disease
Cognition
Consciousness
Coronavirus
Covid
Cryotherapy
Depression
Deuterium
Diet
Dietary Guidelines
EMFs
Emotions
Endocrine Disruptors
Environment
Exercise
Farming
Fasting
Fats
Fluoride
Food
Food Like Product
Food-like Product
Forest
Gardening
Genetics
Glyphosate
GMOs
Hamstrings
Healing
Health
Herbalism
Hormones
HRV
Immunity
Infertility
Laughter
Lockdowns
Loneliness
Longevity
Masks
Meditation
Metabolism
Microbiome
Microwave Radiation
Mind
Mortality
Musculoskeletal System
Nature
Neuroplasticity
Nutrition
Omega 3
Omega-3
Organic
Pelvis/Thigh
Pesticides
Physical Therapy
Placebo
Pollution
Positive
Pregnancy
Prevention
Processed Foods
Psi
Quadriceps
Research
Retirement
Salt
Sleep
Spine/Thorax
Spirit
Stress
Sugar
Technology
Touch Screens
Toxicity
Vaccines
Well Being
Well-Being
 RSS Feed
RSS Feed





