Given that neural plasticity is at its greatest during infancy and toddlerhood, sleep is likely to have the most impact on the brain and on cognition during this critical period of early development. Yet, around 20–30% of young children experience problems with sleep. Researchers have observed that even though some infants with atypical sleep patterns early on eventually develop typical patterns of sleep by 6 or 7 years of age, reduced sleep duration in the first two years of life may have long-term consequences on later developmental outcomes, such as some degree of impaired physical, emotional and social functioning. A growing body of evidence suggests that children and adolescents displaying sleep difficulties or irregular bedtime is significantly associated with later problems of mental and physical health and lower cognitive and academic performance (Hill, Hogan, & Karmiloff-Smith, 2007; Kelly, Kelly, & Sacker, 2013; Magee, Gordon, & Caputi, 2014; Lam, Hiscock, & Wake, 2003; Wake, et al., 2006). For infants and toddlers, touchscreen devices offer an attractive source of stimulation, and their portability allows for a wide range of use across multiple settings. However, the widespread use of devices in this age group has raised serious concerns for parents, educators and policy makers, as the potential impact of touchscreen use on toddler development, such as sleep, remains unknown. In addition, research into the long-term impact of poor sleep during early development remains limited. Yet, findings so far coincide, linking shorter sleep duration to negative developmental outcomes. The majority of studies (~90%) show a consistent pattern linking increased screen time with shorter total sleep time and delayed bedtime. As a result, recent guidelines have recommended screens to be kept out of a child’s bedroom specifically because of the potential impact they may have on sleep (OfCom, 2014). Given the evidence that:
A recent meta-analytic review identified 20 studies in children and adolescents aged between 6 and 19, and found strong and consistent evidence for detrimental effects of portable touchscreen devices on sleep quality and quantity (Carter, Rees, Hale, Bhattacharjee, & Paradkar, 2016). All studies used parent questionnaires, and have reported a significant effect of screen time on sleep: increased amount of TV viewing was associated with parent-reported sleep problems, shorter night-time sleep duration, reduced quality of sleep, and irregular naptime and bedtime schedules, adjusting for known confounds including socioeconomic status (SES). Using a large scale survey, researchers have started to investigate the relationship between touchscreen use and sleep in infants and toddlers between 6 and 36 months of age. Parents were asked to report on the average duration of their child’s daytime and night-time sleep, the time taken for their child to fall asleep, as well as the frequency of night awakenings, to obtain a comprehensive account of infant/toddler sleep patterns. The UK-based survey on 715 families, reported that 75% of toddlers between 6 months and 3 years of age use a touchscreen on a daily basis. The researchers found that the prevalence of daily use increases substantially with age, from 51% in 6- to 11-month-old infants to 92.05% by 25–36 months. Among users, daily usage increased with age from 8.53 minutes a day (6–11 months) to 45 minutes a day (26–36 months). The average touchscreen usage in this sample is 24.44 minutes. There was a significant association between touchscreen use and duration of sleep at night, and sleep onset (the type it takes to falls asleep), with increased touchscreen use associated with decreased night-time sleep, increased daytime sleep and a longer sleep onset. There was no significant association between touchscreen usage and frequency of night awakenings. Results also showed that increased touchscreen use was associated with decreased overall amount of sleep. The researchers concluded that every additional hour of touchscreen use is associated with an overall reduction in sleep of 15.6 minutes. The blue wavelengths emitted by electronic devices—which are beneficial during daylight hours because they boost attention, reaction times, and mood—seem to be the most disruptive at night. While light of any kind can suppress the secretion of melatonin, blue light at night does so more powerfully. Researchers conducted an experiment comparing the effects of 6.5 hours of exposure to blue light to exposure to green light of comparable brightness. The blue light suppressed melatonin for about twice as long as the green light and shifted circadian rhythms by twice as much (3 hours vs. 1.5 hours). (Harvard, 2015). It is worth noting that touchscreen use may also have positive effect on some aspects of development. In a recent study of the same sample of infants and toddlers, increased active touchscreen use was associated with earlier achievement in fine motor milestones (Bedford, Saez de Urabain, Cheung, Karmiloff-Smith & Smith, 2016). Together, these findings emphasize the need for a more in-depth understanding of how to maximize benefits and minimize negative consequences of this modern technology. ReferencesBedford, R., Saez de Urabain, I. R., Cheung, C. H., Karmiloff-Smith, A. & Smith, T. J. (2016).
Toddlers’ Fine Motor Milestone Achievement Is Associated with Early Touchscreen Scrolling. Front Psychol 7, 1108, https://doi.org/10.3389/fpsyg.2016.01108 Carter, B., Rees, P., Hale, L., Bhattacharjee, D. & Paradkar, M. S. (2016). Association Between Portable Screen-Based Media Device Access or Use and Sleep Outcomes: A Systematic Review and Meta-analysis. JAMA Pediatr, https://doi.org/10.1001/jamapediatrics.2016.2341 Cheung, C., Bedford, R., Saez De Urabain, I., Karmiloff-Smith, A. and Smith, T. (2017). Daily touchscreen use in infants and toddlers is associated with reduced sleep and delayed sleep onset. Scientific Reports, 7, p.46104. https://doi.org/10.1038/srep46104 Harvard (2015). Blue light has a dark side - Harvard Health. [online] Harvard Health. Available at: https://www.health.harvard.edu/staying-healthy/blue-light-has-a-dark-side [Accessed 3 Oct. 2017]. Hill, C. M., Hogan, A. M. & Karmiloff-Smith, A. (2007). To sleep, perchance to enrich learning? Arch Dis Child 92, 637–643, https://doi.org/10.1136/adc.2006.096156 Kelly, Y., Kelly, J. & Sacker, A. (2013). Time for bed: associations with cognitive performance in 7-year-old children: a longitudinal population-based study. J Epidemiol Community Health 67, 926–931, https://doi.org/10.1136/jech-2012-202024 Magee, C. A., Gordon, R. & Caputi, P. (2014). Distinct developmental trends in sleep duration during early childhood. Pediatrics 133, e1561–1567, https://doi.org/10.1542/peds.2013-3806 Lam, P., Hiscock, H. & Wake, M. (2003). Outcomes of infant sleep problems: a longitudinal study of sleep, behavior, and maternal well-being. Pediatrics 111, e203–207 OfCom. Children and Parents: Media Use and Attitudes Report. (2014). Available at https://www.ofcom.org.uk/__data/assets/pdf_file/0027/76266/childrens_2014_report.pdf Wake, M. et al. (2006). Prevalence, stability, and outcomes of cry-fuss and sleep problems in the first 2 years of life: prospective community-based study. Pediatrics 117, 836–842, https://doi.org/10.1542/peds.2005-0775
0 Comments
Fabric softeners were designed to free your clothes of both wrinkles and static cling, and give them a fresh fragrance. Therefore when people use fabric softeners and dryer sheets, they are coating their cloths with a thin film of artificial chemical perfumes and plasticizers that will be easily transferred to their skin the next time they put on those cloths, especially when one begins to perspire. Nearly every chemical that touches the skin finds its way into the body and into the bloodstream. The wetter your body becomes, the more easily the chemicals can move from clothing into your skin. And since many of these chemical compounds are by themselves solvents, they are rather good at moving through cellular membranes and entering tissues of the body, including nervous system tissues. In addition, just like other perfumes, a person’s sensitivity to these perfumes decreases over time to the point where they don’t even notice how potent these artificial fragrance chemicals are. Furthermore, when consumers use dryer sheets, those chemicals are heated and then shot into the air for you to breathe into your lungs. What amalgamation of ingredients have the teams of scientists concocted in laboratories to bring you these indulgences? And how toxic are they? Volatile Indoor Pollutants Though these products are approved by the U.S. Environmental Protection Agency (EPA), fabric softeners may top the list as one of the worst "indoor pollutants". In a controlled study of washing and drying laundry, researchers sampled emissions from residential dryer vents during the use of no products, fragranced detergent, and fragranced detergent plus fragranced dryer sheet. The researchers found more than 25 volatile organic compounds (VOC) emitted from dryer vents, with the highest concentrations of acetaldehyde, acetone, and ethanol. Seven of these VOCs are classified as hazardous air pollutants (HAPs) and two as carcinogenic HAPs (acetaldehyde and benzene) with no safe exposure level, according to the US Environmental Protection Agency (Steinemann et al., 2011). Cationic Fabric Softener: Known Asthmagen Cationic fabric softeners are considered to be asthmagens. In laboratory testing in which mice breathed the dilute volatile emissions of air fresheners, fabric softeners, colognes, and mattresses for 1 h, we measured various combinations of sensory irritation, pulmonary irritation, airflow limitation (analogous to asthma attacks), and neurotoxicity. The same effects were observed after mice were subjected to inhale air samples taken from sites associated with repeated human complaints of poor air quality (Anderson & Anderson, 1999). Not everyone may suffer an allergic reaction by being exposed to cationic fabric softeners. But it should be noted that long-term effects have not been adequately studied for them to be deemed as safe and effective. Fragrance: Any Number of Synthetic Chemicals Although all other ingredients in your personal care products must be disclosed on the label by specific name, the so-called “fragrance loophole” in federal labeling law means that ingredients added to provide a pleasant scent, or to mask a bad one, need only be listed under the generic term “fragrance.” The International Fragrance Association, an industry trade group, publishes an online “Transparency List” of nearly 4,000 ingredients that manufacturers say they use in formulas for consumer products under the ingredient "fragrance". Some common culprits include:
It has been established that many of the fragrance ingredients, especially fragrance mixtures, have been identified as allergens. Thus, a person exposed to a certain fragrance material will elicit an allergic response when exposed to this fragrance from any product whether cosmetic or detergents under similar exposure conditions (Europa.eu, 2002). Phthalates: Endocrine Disruptors and Lowers IQ Phthalates ("Thal-ates") are mainly used as a plasticizer - which is an additive that increases the plasticity or viscosity of a material. Phthalates are weak endocrine disruptors and androgen blocking chemicals. In other words, these chemicals, when absorbed into the body, can either mimic or block female hormones, or in males, suppress the hormones involved in male sexual development. In lab animals, phthalate exposure has been found to be associated with numerous reproductive health and developmental problems such as:
There is no easy way to tell if a product has added phthalates. Phthalates can be identified on labels by a three or four letter acronym that defines their chemical structures. Labels rarely state “contains phthalates”. Phthalates are used in a wide range of common (especially plastic) products, including but not limited to:
People are exposed to phthalates by touching, eating, and/or drinking products that have been in contact with containers and products containing phthalates. To a lesser extent, exposure can occur from breathing in air that contains phthalate vapors or dust contaminated with phthalate particles. Due to the ubiquity of plastics (and therefore plasticizers) in modern life, the vast majority of people are exposed to phthalates, and most Americans tested by the have metabolites of multiple phthalates in their urine, according to the Centers for Disease Control and Prevention (CDC, 2009). Researchers have observed that children who experienced prenatal exposure to elevated levels of phthalates had lower IQ scores than children exposed to lower levels. The new research adds to a body of evidence regarding the association between prenatal exposure to phthalates and problems with cognitive function and behavior. During the third trimester of pregnancy, the researchers measured urinary metabolites of four phthalates: di-n-butyl phthalate (DnBP), di-isobutyl phthalate (DiBP), di-2-ethylhexyl phthalate, and diethyl phthalate. At age 7, the children of the mothers with the highest concentrations of DnBP and DiBP metabolites had IQs 6.6 and 7.6 points lower, respectively, than children of mothers exposed to the lowest concentrations. Other research has shown that a six- or seven-point decline in IQ can substantially affect academic achievement and occupational potential (Factor-Litvak, 2014). A separate study examined cognitive function in relation to pre-and postnatal phthalate exposure in children 2–12 years old. After recruiting 430 pregnant women in their third trimester in Taichung, Taiwan from 2001–2002. A total of 110, 79, 76, and 73 children were followed up at ages 2, 5, 8, and 11, respectively. The children’s cognitive function was evaluated at four different time points using different tests for assessing neurocognitive functions and intelligence (IQ). Urine samples were collected from mothers during pregnancy and from children at each follow-up visit. They were analyzed for seven metabolite concentrations of widely used phthalate esters. The researchers found significant inverse associations between the children’s levels of urinary phthalate levels and their IQ scores, after controlling for maternal phthalate levels and potential confounding variables. Phthalate exposure was associated with decreased cognitive development in the young children (Huang et al., 2015). A Healthy Fabric Softener Alternative Ingredients:
Tips to Avoid Toxic Chemical Products
References Anderson, R. C., & Anderson, J. H. (1999). Sensory irritation and multiple chemical sensitivity. Toxicology and Industrial Health, 15(3-4), 339-45. http://dx.doi.org/10.1191/074823399678846817
CDC. (2009). Phthalates. [online] Available at: https://www.cdc.gov/biomonitoring/pdf/Pthalates_FactSheet.pdf [Accessed 29 Sep. 2017]. Europa.eu. (2002). The Scientific Committee on Cosmetic Products and Non-Food Products Intended for Consumers.. [online] Available at: http://ec.europa.eu/health/ph_risk/committees/sccp/documents/out171_en.pdf [Accessed 30 Sep. 2017]. Factor-Litvak P, Insel B, Calafat AM, Liu X, Perera F, Rauh VA, Whyatt RM. 2014. Persistent associations between maternal prenatal exposure to phthalates on child IQ at age 7 years. PLoS One 9(12):e114003. Huang, H., Chen, H., Su, P., Huang, P., Sun, C., Wang, C., Chen, H., Hsiung, C. and Wang, S. (2015). Fetal and Childhood Exposure to Phthalate Diesters and Cognitive Function in Children Up to 12 Years of Age: Taiwanese Maternal and Infant Cohort Study. PLOS ONE, 10(6), p.e0131910. IFRA International Fragrance Association. (2015). Ingredients transparancy list. [online] Available at: http://www.ifraorg.org/en-us/ingredients#.U9qfRoBdVss [Accessed 30 Sep. 2017]. National Institute of Health. (2017). Phthalates: The Everywhere Chemical. [online] Available at: https://www.niehs.nih.gov/research/supported/assets/docs/j_q/phthalates_the_everywhere_chemical_handout_508.pdf [Accessed 30 Sep. 2017]. Steinemann, A., Gallagher, L., Davis, A. and MacGregor, I. (2011). Chemical emissions from residential dryer vents during use of fragranced laundry products. Air Quality, Atmosphere & Health, 6(1), pp.151-156. https://doi.org/10.1007/s11869-011-0156-1
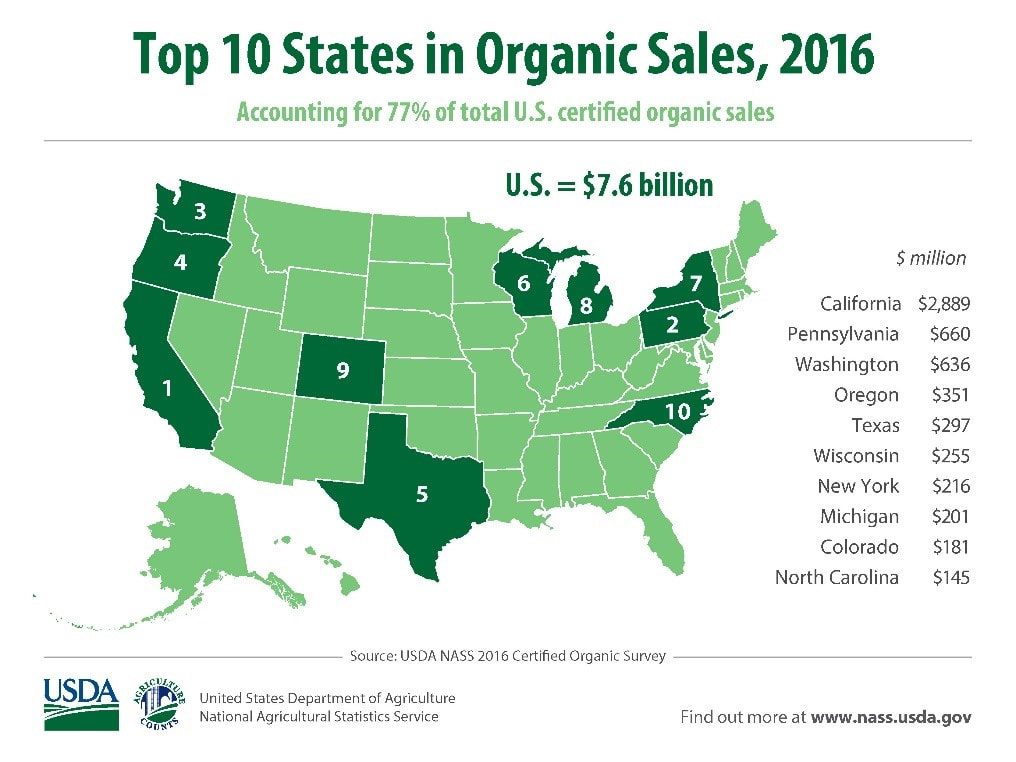
California, with $2.9 billion in certified organic sales, continued to lead the nation in certified sales, accounting for 38% of the U.S. total. It also had the largest share of certified organic acres and farms. Ten states accounted for 77% of U.S. certified organic sales, which was virtually the same share compared to 2015 and 2014. The results from the survey also included:
The top organic commodities in 2016 were:
Other top organic crops were strawberries, grapes, tomatoes, corn, potatoes, hay, spinach, and mushrooms. The survey is a census of all known U.S. farmers and ranchers with certified organic production in 2016. Producers must meet the standards set out by USDA’s Agricultural Marketing Service’s National Organic Program and be certified compliant by an approved agent of the program. ReferencesNASS & USDA (2017). 2016 Sales of U.S. Certified Organic Agricultural Production Up 23 Percent from Previous Year. [online] Available at: https://www.nass.usda.gov/Newsroom/2017/09_20_2017.php [Accessed 28 Sep. 2017].
USDA. (2017). Certified Organic Survey. [online] Available at: http://usda.mannlib.cornell.edu/usda/nass/OrganicProduction//2010s/2017/OrganicProduction-09-20-2017.pdf [Accessed 28 Sep. 2017].
The Prospective Urban Rural Epidemiology (PURE) study is a large, epidemiological study that included more than 135,000 individuals between the ages of 35–70 years across 18 countries. Regions included Canada, Sweden, United Arab Emirates, Argentina, Brazil, Chile, China, Colombia, Iran, Malaysia, occupied Palestinian territory, Poland, South Africa, Turkey, Bangladesh, India, Pakistan, and Zimbabwe. Overall, the researchers found that high carbohydrate intake (more than 60% of energy) was associated with higher risk of total mortality, whereas total fat and individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an inverse association with stroke. For decades, dietary guidelines have focused on reducing total fat and saturated fatty acid intake, based on the presumption that replacing saturated fatty acids with carbohydrate and unsaturated fats will lower LDL cholesterol and should therefore reduce cardiovascular disease events. This focus is largely based on selective emphasis on some observational and clinical data, despite the existence of several randomized trials and observational studies that do not support these conclusions. Results of the Study After documenting 5796 deaths and 4784 major cardiovascular disease events and running statistical analyses, the researchers observed:
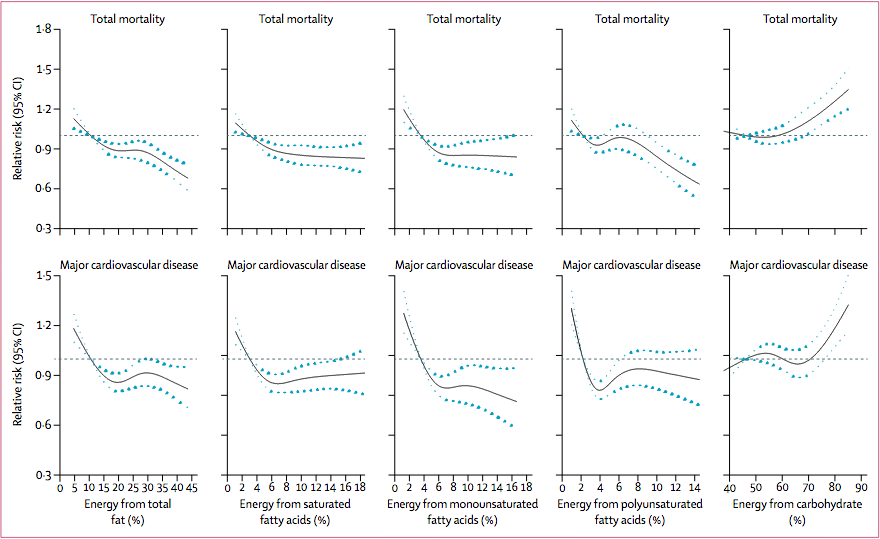 Association between estimated percentage energy from nutrients and total mortality and major cardiovascular disease (n=135335). Image from (Dehghan et al., 2017) Recommendations and Take Away The results of this study do not suggest a low-carbohydrate diet, but rather that a total fat intake of about 35% of energy while lowering carbohydrate intake might lower risk of total mortality. Collectively, the data does not support the recommendation to limit saturated fatty acids to less than 10% of intake and that a very low intake (ie, below about 7% of energy) might even be harmful. Limitations of the Study
The researchers declare no conflicts of interests References Brown, E. (2017). More Evidence That Everything the Government Teaches Us About Eating Is Wrong. [online] Reason.com. Available at: http://reason.com/blog/2017/08/30/pure-study-challenges-dietary-dogma [Accessed 20 Sep. 2017].
Dehghan, M., Mente, A., Zhang, X., Swaminathan, S., Li, W., Mohan, V., Iqbal, R., Kumar, R., Wentzel-Viljoen, E., Rosengren, A., Amma, L., Avezum, A., Chifamba, J., Diaz, R., Khatib, R., Lear, S., Lopez-Jaramillo, P., Liu, X., Gupta, R., Mohammadifard, N., Gao, N., Oguz, A., Ramli, A., Seron, P., Sun, Y., Szuba, A., Tsolekile, L., Wielgosz, A., Yusuf, R., Hussein Yusufali, A., Teo, K., Rangarajan, S., Dagenais, G., Bangdiwala, S., Islam, S., Anand, S., Yusuf, S., Diaz, R., Orlandini, A., Linetsky, B., Toscanelli, S., Casaccia, G., Cuneo, J., Rahman, O., Yusuf, R., Azad, A., Rabbani, K., Cherry, H., Mannan, A., Hassan, I., Talukdar, A., Tooheen, R., Khan, M., Sintaha, M., Choudhury, T., Haque, R., Parvin, S., Avezum, A., Oliveira, G., Marcilio, C., Mattos, A., Teo, K., Yusuf, S., Dejesus, J., Agapay, D., Tongana, T., Solano, R., Kay, I., Trottier, S., Rimac, J., Elsheikh, W., Heldman, L., Ramezani, E., Dagenais, G., Poirier, P., Turbide, G., Auger, D., De Bluts, A., Proulx, M., Cayer, M., Bonneville, N., Lear, S., Gasevic, D., Corber, E., de Jong, V., Vukmirovich, I., Wielgosz, A., Fodor, G., Pipe, A., Shane, A., Lanas, F., Seron, P., Martinez, S., Valdebenito, A., Oliveros, M., Wei, L., Lisheng, L., Chunming, C., Xingyu, W., Wenhua, Z., Hongye, Z., Xuan, J., Bo, H., Yi, S., Jian, B., Xiuwen, Z., Xiaohong, C., Tao, C., Hui, C., Xiaohong, C., Qing, D., Xiaoru, C., Qing, D., Xinye, H., Bo, H., Xuan, J., Jian, L., Juan, L., Xu, L., Bing, R., Yi, S., Wei, W., Yang, W., Jun, Y., Yi, Z., Hongye, Z., Xiuwen, Z., Manlu, Z., Fanghong, L., Jianfang, W., Yindong, L., Yan, H., Liangqing, Z., Baoxia, G., Xiaoyang, L., Shiying, Z., Rongwen, B., Xiuzhen, T., Dong, L., Di, C., Jianguo, W., Yize, X., Tianlu, L., Peng, Z., Changlin, D., Ning, L., Xiaolan, M., Yuqing, Y., Rensheng, L., Minfan, F., Jing, H., Yu, L., Xiaojie, X., Qiang, Z., Lopez-Jaramillo, P., Lopez, P., Garcia, R., Jurado, L., Gómez-Arbeláez, D., Arguello, J., Dueñas, R., Silva, S., Pradilla, L., Ramirez, F., Molina, D., Cure-Cure, C., Perez, M., Hernandez, E., Arcos, E., Fernandez, S., Narvaez, C., Paez, J., Sotomayor, A., Garcia, H., Sanchez, G., David, T., Rico, A., Mony, P., Vaz, M., Bharathi, A., Swaminathan, S., Kurpad, K., Jayachitra, K., Kumar, N., Hospital, H., Mohan, V., Deepa, M., Parthiban, K., Anitha, M., Hemavathy, S., Rahulashankiruthiyayan, T., Anitha, D., Sridevi, K., Gupta, R., Panwar, R., Mohan, I., Rastogi, P., Rastogi, S., Bhargava, R., Kumar, R., Thakur, J., Patro, B., Lakshmi, P., Mahajan, R., Chaudary, P., Kutty, V., Vijayakumar, K., Ajayan, K., Rajasree, G., Renjini, A., Deepu, A., Sandhya, B., Asha, S., Soumya, H., Kelishadi, R., Bahonar, A., Mohammadifard, N., Heidari, H., Yusoff, K., Ismail, T., Ng, K., Devi, A., Nasir, N., Yasin, M., Miskan, M., Rahman, E., Arsad, M., Ariffin, F., Razak, S., Majid, F., Bakar, N., Yacob, M., Zainon, N., Salleh, R., Ramli, M., Halim, N., Norlizan, S., Ghazali, N., Arshad, M., Razali, R., Ali, S., Othman, H., Hafar, C., Pit, A., Danuri, N., Basir, F., Zahari, S., Abdullah, H., Arippin, M., Zakaria, N., Noorhassim, I., Hasni, M., Azmi, M., Zaleha, M., Hazdi, K., Rizam, A., Sazman, W., Azman, A., Khatib, R., Khammash, U., Khatib, A., Giacaman, R., Iqbal, R., Afridi, A., Khawaja, R., Raza, A., Kazmi, K., Zatonski, W., Szuba, A., Zatonska, K., Ilow, R., Ferus, M., Regulska-Ilow, B., Rózanska, D., Wolyniec, M., Alkamel, Ali, M., Kruger, M., Voster, H., Schutte, A., Wentzel-Viljoen, E., Eloff, F., de Ridder, H., Moss, H., Potgieter, J., Roux, A., Watson, M., de Wet, G., Olckers, A., Jerling, J., Pieters, M., Hoekstra, T., Puoane, T., Igumbor, E., Tsolekile, L., Sanders, D., Naidoo, P., Steyn, N., Peer, N., Mayosi, B., Rayner, B., Lambert, V., Levitt, N., Kolbe-Alexander, T., Ntyintyane, L., Hughes, G., Swart, R., Fourie, J., Muzigaba, M., Xapa, S., Gobile, N., Ndayi, K., Jwili, B., Ndibaza, K., Egbujie, B., Rosengren, A., Boström, K., Gustavsson, A., Andreasson, M., Snällman, M., Wirdemann, L., Oguz, A., Imeryuz, N., Altuntas, Y., Gulec, S., Temizhan, A., Karsidag, K., Calik, K., Akalin, A., Caklili, O., Keskinler, M., Erbakan, A., Yusufali, A., Almahmeed, W., Swidan, H., Darwish, E., Hashemi, A., Al-Khaja, N., Muscat-Baron, J., Ahmed, S., Mamdouh, T., Darwish, W., Abdelmotagali, M., Awed, S., Movahedi, G., Hussain, F., Al Shaibani, H., Gharabou, R., Youssef, D., Nawati, A., Salah, Z., Abdalla, R., Al Shuwaihi, S., Al Omairi, M., Cadigal, O., Alejandrino, R., Chifamba, J., Gwaunza, L., Terera, G., Mahachi, C., Murambiwa, P., Machiweni, T. and Mapanga, R. (2017). Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. The Lancet. http://dx.doi.org/10.1016/S0140-6736(17)32252-3 From Mercola: Researchers have established that processed food is addictive, can make you extremely unhappy and will prematurely kill you. Is there a chance that food manufacturers been able to deceive the world about these facts? Dr. Robert Lustig has written a new book, “The Hacking of the American Mind: The Science Behind the Corporate Takeover of Our Bodies and Brains,” in which he explains how and why this occurred. He is perhaps most well-known for his brilliant research into sugar and obesity, and his previous book, “Fat Chance: Beating the Odds Against Sugar, Processed Food, Obesity and Disease,” was a New York Times Best Seller. Lustig is an emeritus professor of pediatrics in the division of endocrinology at the University of California, San Francisco, a member of the Institute for Health Policy Studies, and he’s also completed a master’s in public health law. Tryptophan, which is the precursor for serotonin, is one of the rarest amino acids in our diet. But it’s a mistake to think the answer to depression is as simple as taking tryptophan to boost serotonin. The reason for this is because most of the tryptophan is converted to serotonin in your gut, and it does not freely travel into your brain. Lustig explains: “Tryptophan is the only amino acid that can be converted into serotonin. Tryptophan is the rarest amino acid in our diet. Eggs have the most. Certain poultry and other avian species have some [tryptophan]. There’s very little in vegetables. Obviously, carbohydrates have virtually no tryptophan whatsoever. It’s actually pretty hard to get tryptophan into your body to start with. Take processed food on top of that, then it’s even harder because it tends to be tryptophan-depleted. [Moreover], 99.9 percent of the tryptophan you ingest either gets turned into serotonin in the gut for your gut’s purposes, or it goes into your platelets to help your platelets help you clot. [So] very little tryptophan actually gets to the brain. Top that off with the fact that tryptophan has to share an amino acid transporter with two relatively common amino acids: phenylalanine and tyrosine, which, by the way, are the precursors for dopamine. You can see that the more processed food you eat, the more dopamine you will make because you will have the precursors for that. They will actually crowd out the ability to get tryptophan across the blood-brain barrier … Yet, serotonin is the nidus of contentment, of happiness. It explains why diet is so problematic … ” Manifesting Happiness Many try to bolster their happiness through certain food choices, but this actually does not work, and Lustig provides compelling arguments that the foods you crave drive up dopamine and drive down serotonin. Rather, it’s experiences that make you happy. People can make you happy. You can make yourself happy. In his book, Lustig outlines a number of different strategies to become happier. “Ultimately, the goal is [to increase] your serotonin,” he says. There are four ways to boost your serotonin, and they’re all free. They’re also things your grandmother likely told you to do. First and foremost is making human connections. “Turns out that Facebook does not count as connection. When we’re talking about interpersonal connection, we’re talking about eye-to-eye,” Lustig says. “The facial emotions of the person you’re talking with activate a set of neurons in your brain called ‘mirror neurons,’ which are the drivers of empathy and specifically linked to serotonin.To be able to generate a feeling of empathy, which ultimately turns into contentment/happiness, you actually have to connect. You can’t do it over the internet. You can’t have a connection with ‘anonymous.’ It just doesn’t work.” On the contrary, social media generate dopamine, associated with pleasure, and hence can drive addiction. The main problem is that when dopamine goes up, serotonin goes down. So, online communication is actually a major causative factor of unhappiness. Lustig also elaborates on how companies — both food manufacturers and electronics companies — capitalize on the biology of dopamine versus serotonin to get us addicted to their products. There’s even a book on this topic written by Nir Eyal, called, “Hooked: How to Build Habit-Forming Products.” Dopamine Versus Serotonin It’s important to realize that the dopamine (or reward-generating) pathway is the same no matter what your source of pleasure is. It can be a substance, such as nicotine, alcohol, heroin or junk food; or it can be behavior, such as internet surfing, shopping or pornography. The problem, in a nutshell, is that dopamine is an excitatory neurotransmitter, and in excess is neurotoxic. When dopamine is released, and the neuron on the other side accepts the signal, it can damage that neuron. Over time, excitatory neurotransmitters can cause cell death. To protect itself from damage, the postsynaptic neuron employs a self-protective mechanism — it downregulates its receptors. By having fewer receptors, the dopamine cannot do as much damage. So, each time you get a “hit” or rush of dopamine, the number of receptors decrease. As a result, you need increasingly larger doses or “hits” to get the same rush. Eventually, you end up with tolerance, a state where even a large dose produces no effect. Once the neurons start to actually die off, you’re a full-blown addict. “The point that you need to know is that it takes three weeks for the receptors to repopulate. The cravings can go on for upwards of a year when you’re addicted. This is a long-term process that sometimes requires medical intervention and medical management by physicians who understand addiction medicine,” Lustig says. Serotonin, on the other hand, is not an excitatory neurotransmitter. When it acts on the serotonin-1a receptor (the “contentment” receptor), no damage occurs. Hence, happiness does not lead to addictive behavior. Keep in mind that dopamine downregulates serotonin, so it’s basically impossible to achieve happiness (related to serotonin) through pleasure-seeking behavior (related to dopamine). One of the cheapest pleasures that stimulates dopamine is sugar. Many reach for sweet junk food when they feel down, thinking it’ll help them feel better, but neurochemical science reveals this simply cannot happen. Add the stress hormone cortisol to the mix, which downregulates the serotonin-1a receptor, and you have a recipe for both addiction and depression. “That’s what we’re seeing throughout all of civilized society, not just in America, but around the world,” Lustig says. Boosting Serotonin There are three other ways, besides connecting, that boost serotonin and happiness. The remaining three of the four C’s are: 1. Contribute: Meaning the act of contributing to something greater than yourself; making a contribution to society. “You can get happiness and contentment from your job, but there are certain criteria that have to be met,” Lustig says. “Most people, unfortunately, have a boss who is not contributing to their happiness. The workplace is not usually the best place to achieve meaningful contentment.” 2. Cope: Lack of sleep, insufficient exercise and multitasking are all causes of unhappiness. Sleep is extremely important for healthy serotonin production. Here, avoiding exposure to electronic screens is important, as blue light inhibits melatonin production, thereby making sleep more elusive. Electronics will also disrupt your sleep and deteriorate your health by exposing you to unnecessary microwaves, discussed in this recent article on depression. 3. Cook: If you cook, you’re likely going to increase your tryptophan, reduce your refined sugar intake, and increase your omega-3 fats (anti-inflammatory) and fiber. Overall, this will result in improved gut health, which has tremendous impact on your mood and mental health. “Numerous investigators … have shown that your gastrointestinal flora tell your brain what they want through signals that go through the bloodstream, and potentially even neural ones as well. If you do not feed your bacteria, you cannot get happy. Eating real food you prepare yourself is super important,” Lustig says. The High Cost of Added Sugar Processed fructose, mostly in the form of corn syrup, has become a major contributor to the $3 trillion health care budget in the United States, and there’s clear data linking sugar consumption to de novo lipogenesis — a disease process associated with fat accumulation in the liver, causing insulin resistance, hyperinsulinemia, metabolic syndrome and associated diseases. That includes Type 2 diabetes, hypertension, lipid problems, cardiovascular disease, cancer and dementia. “We have the mechanism by which this occurs. In fact, our paper in Gastroenterology1 demonstrates that if you take sugar out of the diet of children with metabolic syndrome and substitute starch — calorie for calorie exchange, glucose for fructose exchange with no change in calories … — in 10 days, you can reverse metabolic syndrome. You can reverse the insulin resistance. You can reverse the liver fat. You can reverse the burden on the pancreas. Basically, all of the metabolic perturbations go away. This is the smoking gun,” Lustig says. “In addition, we have a paper in BMJ Open2 which models what could happen in terms of health care expenditures and disease rates if we reduced our sugar consumption by 20 percent, which is what taxes would do. Or if we reduce sugar consumption by 50 percent (which is what the United States Department of Agriculture suggested we do), for nonalcoholic fatty liver disease alone … the United States, over the next 20 years, could save $103 billion, just on that disease alone. Ultimately, this is where the money goes. This is why health care will be defunct. This is why Medicare will be broke by the year 2026 … We have to deal with health. Health is going down the tubes. There’s no amount of health care that can fix what’s wrong with our diet, unless we fix the diet first … The bottom line is we are in trouble. But you can’t fix a problem until you recognize what the problem is. This book, ‘The Hacking of the American Mind,’ demonstrates how the science, how the biology, ultimately has influenced not just our health, but in fact, our policy.” A Solution: Eat Real Food As mentioned, a big part of the happiness equation is to increase serotonin by optimizing tryptophan. However, the dilemma is that most of the serotonin produced in the gut is used there locally. It does not enter your brain. Lustig explains: “There are many diversions for tryptophan away from the brain. It can be metabolized in the intestine itself. It can be metabolized in the platelets. It can be turned into kynurenine, which is a secondary metabolite in the liver. It may not be transported across the blood-brain barrier because of phenylalanine and tyrosine taking up the aromatic amino acid transporter. In addition, of course, your serotonin neurons must be functional. There are things that will kill off serotonin neurons, including party drugs. For instance, MDMA, or Ecstasy, is a famous dopamine and serotonin killer … Once you’ve lost those serotonin neurons, it’s pretty hard to get any sort of happiness signal.” So, how do you boost systemic tryptophan? One of the keys is to eat real food, and to make sure you include high-tryptophan foods, the highest of which is egg whites. You also need omega-3 fatty acids, especially DHA, which is a component of every cell in your body. More than 90 percent of the omega-3 fat found in brain tissue is DHA. “Omega-3s are probably the single most beneficial thing you can put in your body. They are anti-inflammatory. They are anti-Alzheimer’s. They increase membrane fluidity. Therefore, they increase neuronal distensibility, which means it’s less likely that any given neuron will die,” Lustig says. “The problem, of course, is that when we took the fat out of the food, we took ALL the fat out of the food. It’s been a real chore to get the medical cognoscenti to turn around on this. I do want to do a shoutout to the American Heart Association, because they have now debunked their long-standing cholesterol-fat hypothesis. They now recognize that saturated fat was not the demon they made it out to be, and that there are seven classes of fats, and that you actually have to consume omega-3s. You have to consume monounsaturated fats. In fact, you do have to consume some saturated fat because it’s a major component of membranes.” ReferencesMercola, J. (2017). How Corporations Took Over Our Bodies and Brains. [online] Mercola.com. Available at: http://articles.mercola.com/sites/articles/archive/2017/09/10/processed-foods-health-effects.aspx [Accessed 11 Sep. 2017].
Ideally, you want your plate to look like a mosaic, painted with various colors from different foods. Create a rainbow of colors on your plate, with fruits and vegetables. Eating a variety of different foods offer more nutrients.
In this powerful TED talk, Dr. William Li discusses the powerful synergistic effects of combining food. |
The Awareness domain contains research, news, information, observations, and ideas at the level of self in an effort to intellectualize health concepts.
The Lifestyle domain builds off intellectual concepts and offers practical applications.
Taking care of yourself is at the core of the other domains because the others depend on your health and wellness.
Archives
May 2024
Categories
All
|



 RSS Feed
RSS Feed





