
Directions
- Answer each question with the response that best fits you. It is recommended that you either photocopy the questionnaires or record your answers on a separate piece of paper. You will hopefully be using them again to test your progress, and it will be easier if you do not have your previous answers in front of you at that point. It is extremely important to answer the questions as accurately and honestly as possible. There are no right or wrong answers. Supply the response that most accurately describes you, not what you think the answer should be. When answering these questions, forget everything you've been told about nutrition. Answer the questions based on your gut instinct to how you would prefer to eat if you could eat what you innately desire.
- Total your scores for each questionnaire. There are numbers in parentheses after each answer. Add up the numbers corresponding to each of your responses to get your total score for the section.
- Graph your scores.
- Calculate your total score by adding up the scores for each section.
You Are What You Eat
Do you shop for food less frequently than every four days?
_____ Yes (1)
_____ No (0)
Do you eat more packaged (frozen or canned) fruits and vegetables than fresh?
_____ Yes (3)
_____ No (0)
Do you eat more cooked vegetables than raw?
_____ Yes (3)
_____ No (0)
Do you eat vegetables with fewer than two meals daily?
_____ Yes (5)
_____ No (0)
Do you buy more non-organic vegetables than organic vegetables?
_____ Yes (5)
_____ No (0)
How often do you use a microwave oven?
_____ Never or very rarely (0)
_____ 1-2 times per week (2)
_____ 3-4 times per week (5)
_____ 4+ times per week (10)
Do you eat white bread more often than whole grain breads?
_____ Yes (5)
_____ No (0)
Do you eat quick cook grains such as Quaker Oats or Minute rice more often than slow cooked organic whole grains?
_____ Yes (5)
_____ No (0)
How often do you consume pasteurized, homogenized milk or cheeses?
_____ Never or very rarely (0)
_____ 1-2 times per week (1)
_____ 3 times per week (3)
_____ 3+ times per week (5)
How often do you eat non-organic yogurts?
_____ Never or very rarely (0)
_____ 1-2 times per week (1)
_____ 3 times per week (3)
_____ 3+ times per week (5)
Do you eat typical store-bought eggs from cage-raised chickens (as opposed to eggs from free-range or pasture-raised chickens)?
_____ Yes (5)
_____ No (0)
Do you eat non-organic red meat more than once every four days?
_____ Yes (3)
_____ No (0)
Do you commonly eat meats (beef, chicken, turkey) from sources other than a free-range and hormone-free source?
_____ Yes (3)
_____ No (0)
Do you eat canned fish more frequently than fresh fish?
_____ Yes (3)
_____ No (0)
How often do you use commercial salad dressings?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ Twice per week (2)
_____ 2+ times per week (3)
How often do you use products containing hydrogenated oils?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ Twice per week (2)
_____ 2+ times per week (5)
Do you eat nuts or seeds that are roasted or salted?
_____ Yes (1)
_____ No (0)
How often do you use white table sugar as a sweetener?
_____ Never or very rarely (0)
_____ Once per week (1)
_____ 2-3 times per week (3)
_____ 3+ times per week (5)
How often do you use artificial sweeteners such as Sweet-n-Low, Equal or NutraSweet?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 2-3 times per week (5)
_____ 3+ times per week (10)
Do you use standard white table salt?
_____ Yes (5)
_____ No (0)
Do you eat TV dinners or highly-processed foods more than three times a week?
_____ Yes (5)
_____ No (0)
How often do you eat from fast food restaurants like McDonalds, TacoBell, Starbucks, etc...?
_____ Never or very rarely (0)
_____ 1-2 times per week (2)
_____ 3 times per week (5)
_____ 3+ times per week (10)
How often do you eat snacks from vending machines?
_____ Never or very rarely (0)
_____ 1-2 times per week (2)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you drink tap water?
_____ Yes (10)
_____ No (0)
How often do you eat some form of store-bought dessert such as ice cream, cookies, donuts, cakes or pies?
_____ Never or very rarely (0)
_____ Once per week (1)
_____ 2-3 times per week (3)
_____ 3+ times per week (5)
_____ Yes (1)
_____ No (0)
Do you eat more packaged (frozen or canned) fruits and vegetables than fresh?
_____ Yes (3)
_____ No (0)
Do you eat more cooked vegetables than raw?
_____ Yes (3)
_____ No (0)
Do you eat vegetables with fewer than two meals daily?
_____ Yes (5)
_____ No (0)
Do you buy more non-organic vegetables than organic vegetables?
_____ Yes (5)
_____ No (0)
How often do you use a microwave oven?
_____ Never or very rarely (0)
_____ 1-2 times per week (2)
_____ 3-4 times per week (5)
_____ 4+ times per week (10)
Do you eat white bread more often than whole grain breads?
_____ Yes (5)
_____ No (0)
Do you eat quick cook grains such as Quaker Oats or Minute rice more often than slow cooked organic whole grains?
_____ Yes (5)
_____ No (0)
How often do you consume pasteurized, homogenized milk or cheeses?
_____ Never or very rarely (0)
_____ 1-2 times per week (1)
_____ 3 times per week (3)
_____ 3+ times per week (5)
How often do you eat non-organic yogurts?
_____ Never or very rarely (0)
_____ 1-2 times per week (1)
_____ 3 times per week (3)
_____ 3+ times per week (5)
Do you eat typical store-bought eggs from cage-raised chickens (as opposed to eggs from free-range or pasture-raised chickens)?
_____ Yes (5)
_____ No (0)
Do you eat non-organic red meat more than once every four days?
_____ Yes (3)
_____ No (0)
Do you commonly eat meats (beef, chicken, turkey) from sources other than a free-range and hormone-free source?
_____ Yes (3)
_____ No (0)
Do you eat canned fish more frequently than fresh fish?
_____ Yes (3)
_____ No (0)
How often do you use commercial salad dressings?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ Twice per week (2)
_____ 2+ times per week (3)
How often do you use products containing hydrogenated oils?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ Twice per week (2)
_____ 2+ times per week (5)
Do you eat nuts or seeds that are roasted or salted?
_____ Yes (1)
_____ No (0)
How often do you use white table sugar as a sweetener?
_____ Never or very rarely (0)
_____ Once per week (1)
_____ 2-3 times per week (3)
_____ 3+ times per week (5)
How often do you use artificial sweeteners such as Sweet-n-Low, Equal or NutraSweet?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 2-3 times per week (5)
_____ 3+ times per week (10)
Do you use standard white table salt?
_____ Yes (5)
_____ No (0)
Do you eat TV dinners or highly-processed foods more than three times a week?
_____ Yes (5)
_____ No (0)
How often do you eat from fast food restaurants like McDonalds, TacoBell, Starbucks, etc...?
_____ Never or very rarely (0)
_____ 1-2 times per week (2)
_____ 3 times per week (5)
_____ 3+ times per week (10)
How often do you eat snacks from vending machines?
_____ Never or very rarely (0)
_____ 1-2 times per week (2)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you drink tap water?
_____ Yes (10)
_____ No (0)
How often do you eat some form of store-bought dessert such as ice cream, cookies, donuts, cakes or pies?
_____ Never or very rarely (0)
_____ Once per week (1)
_____ 2-3 times per week (3)
_____ 3+ times per week (5)
Stress
Do you eat more or less when stressed than when not stressed?
_____ More (10)
_____ Same or less (0)
Do you worry over job, income or money problems?
_____ Yes (10)
_____ No (0)
Are any of your relationships causing you stress?
_____ Yes (10)
_____ No (0)
Do you often feel anxious?
_____ Yes (5)
_____ No (0)
Do you often get upset when things go wrong?
_____ Yes (5)
_____ No (0)
Do you lash out at others?
_____ Yes (5)
_____ No (0)
Do you feel your sex drive is lower than normal for you?
_____ Yes (5)
_____ No (0)
Do you feel isolated or lonely?
_____ Yes (3)
_____ No (0)
Do you feel stressed due to lack of intimacy in one or more relationships?
_____ Yes (5)
_____ No (0)
Have you had reduced contact with friends (feeling antisocial) or an increase in contact because you feel you need to vent your frustrations or stressed to others?
_____ Yes (3)
_____ No (0)
Do you take any form of medication prescribed by a physician directly or indirectly related to stress in your life or for a psychological disorder?
_____ Yes (15)
_____ No (0)
Do you commonly lose more than two fays or work a year due to illness?
_____ Yes (5)
_____ No (0)
_____ More (10)
_____ Same or less (0)
Do you worry over job, income or money problems?
_____ Yes (10)
_____ No (0)
Are any of your relationships causing you stress?
_____ Yes (10)
_____ No (0)
Do you often feel anxious?
_____ Yes (5)
_____ No (0)
Do you often get upset when things go wrong?
_____ Yes (5)
_____ No (0)
Do you lash out at others?
_____ Yes (5)
_____ No (0)
Do you feel your sex drive is lower than normal for you?
_____ Yes (5)
_____ No (0)
Do you feel isolated or lonely?
_____ Yes (3)
_____ No (0)
Do you feel stressed due to lack of intimacy in one or more relationships?
_____ Yes (5)
_____ No (0)
Have you had reduced contact with friends (feeling antisocial) or an increase in contact because you feel you need to vent your frustrations or stressed to others?
_____ Yes (3)
_____ No (0)
Do you take any form of medication prescribed by a physician directly or indirectly related to stress in your life or for a psychological disorder?
_____ Yes (15)
_____ No (0)
Do you commonly lose more than two fays or work a year due to illness?
_____ Yes (5)
_____ No (0)
Sleep Wake Cycles
Do you live in the same time zone you were born in?
_____ Yes (0)
_____ No (5)
Do you travel across time zones more than once a month?
_____ Yes (10)
_____ No (0)
How often do you wake up feeling un-rested and in need of more sleep?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you commonly go to bed after 10:30 p.m.?
_____ Yes (10)
_____ No (0)
Are the times you have bowel movements consistent and predictable on a daily basis?
_____ Yes (0)
_____ No (5)
Do you suffer from reduced memory since moving to a new time zone or since traveling across time zones?
_____ Yes (10)
_____ No (0)
Has your sense of hunger changed from being hungry at breakfast (upon rising), lunch (midday) and dinner times (sunset) since moving to a new time zone or traveling across time zones frequently (more than once a month)?
_____ Yes (10)
_____ No (0)
How often do you wake up at night between 1:00 a.m. and 4:00 a.m. and have a hard time falling back to sleep?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
How often do you tend to have a hard time staying awake in the afternoon after eating lunch?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you do shift work that requires you to stay up late at night?
_____ Yes (10)
_____ No (0)
_____ Yes (0)
_____ No (5)
Do you travel across time zones more than once a month?
_____ Yes (10)
_____ No (0)
How often do you wake up feeling un-rested and in need of more sleep?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you commonly go to bed after 10:30 p.m.?
_____ Yes (10)
_____ No (0)
Are the times you have bowel movements consistent and predictable on a daily basis?
_____ Yes (0)
_____ No (5)
Do you suffer from reduced memory since moving to a new time zone or since traveling across time zones?
_____ Yes (10)
_____ No (0)
Has your sense of hunger changed from being hungry at breakfast (upon rising), lunch (midday) and dinner times (sunset) since moving to a new time zone or traveling across time zones frequently (more than once a month)?
_____ Yes (10)
_____ No (0)
How often do you wake up at night between 1:00 a.m. and 4:00 a.m. and have a hard time falling back to sleep?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
How often do you tend to have a hard time staying awake in the afternoon after eating lunch?
_____ Never or very rarely (0)
_____ Once a week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you do shift work that requires you to stay up late at night?
_____ Yes (10)
_____ No (0)
You Are When You Eat
Do you frequently skip meals?
_____ Yes (3)
_____ No (0)
How often do you typically go more than four hours without eating?
_____ Never or very rarely (0)
_____ 1-2 times per week (1)
_____ 3 times per week (2)
_____ 3+ times per week (3)
How often do you skip breakfast?
_____ Never or very rarely (0)
_____ 2 times per week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you avoid fats when eating?
_____ Yes (5)
_____ No (0)
Do you frequently eat carbohydrates (i.e. breads, bagels, cookies, pasta, fruit, cereals, muffins, crackers, chocolate, or candy) by themselves?
_____ Yes (5)
_____ No (0)
Do you often get hungry or crave sweets within two hours after eating a meal?
_____ Yes (5)
_____ No (0)
How often do you consume drinks containing caffeine or sugar (i.e. coffee, tea, sodas, fruit juices with sucrose, corn syrup or added sugar)?
_____ Never or very rarely (0)
_____ 1 cup per day (1)
_____ 2 cups per day (3)
_____ More than 2 cups per day (5)
Have you tried diets to lose weight?
_____ No (0)
_____ Once (1)
_____ Twice (2)
_____ 3-5 times (5)
_____ More than five times (10)
Do you have difficulty burning fat around your belly, hips or thighs even with regular exercise?
_____ Yes (3)
_____ No (0)
Do you eat your largest meal in the evening?
_____ Yes (1)
_____ No (0)
_____ Yes (3)
_____ No (0)
How often do you typically go more than four hours without eating?
_____ Never or very rarely (0)
_____ 1-2 times per week (1)
_____ 3 times per week (2)
_____ 3+ times per week (3)
How often do you skip breakfast?
_____ Never or very rarely (0)
_____ 2 times per week (1)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you avoid fats when eating?
_____ Yes (5)
_____ No (0)
Do you frequently eat carbohydrates (i.e. breads, bagels, cookies, pasta, fruit, cereals, muffins, crackers, chocolate, or candy) by themselves?
_____ Yes (5)
_____ No (0)
Do you often get hungry or crave sweets within two hours after eating a meal?
_____ Yes (5)
_____ No (0)
How often do you consume drinks containing caffeine or sugar (i.e. coffee, tea, sodas, fruit juices with sucrose, corn syrup or added sugar)?
_____ Never or very rarely (0)
_____ 1 cup per day (1)
_____ 2 cups per day (3)
_____ More than 2 cups per day (5)
Have you tried diets to lose weight?
_____ No (0)
_____ Once (1)
_____ Twice (2)
_____ 3-5 times (5)
_____ More than five times (10)
Do you have difficulty burning fat around your belly, hips or thighs even with regular exercise?
_____ Yes (3)
_____ No (0)
Do you eat your largest meal in the evening?
_____ Yes (1)
_____ No (0)
Digestion
How often do you experience lower abdominal bloating?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you frequently have loose stools or diarrhea?
_____ No (0)
_____ Once a week (1)
_____ 3 or more times per week (5)
How often do you experience constipation or stools that are compact or hard to pass?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 or more times per week (5)
Do you find that you often burp after meals?
_____ Yes (3)
_____ No (0)
Do you frequently have gas?
_____ Yes (3)
_____ No (0)
Do you crave certain foods such as bread, chocolate, certain fruit, and red meat if you have not eaten them in a day or two?
_____ Yes (5)
_____ No (0)
How often do you have a poor appetite or feel worse after eating?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 times per week (5)
_____ 3 or more times per week (10)
Do you have an excessive appetite and/or sweet cravings?
_____ Yes (5)
_____ No (0)
Do you frequently (more than twice a week) experience abdominal pain, cramps or general abdominal discomfort?
_____ Yes (20)
_____ No (0)
How often do you have indigestion, heartburn or an upset stomach?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 times per week (5)
_____ 3 or more times per week (10)
How often do you get a headache after eating?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 or more times per week (5)
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 times per week (5)
_____ 3+ times per week (10)
Do you frequently have loose stools or diarrhea?
_____ No (0)
_____ Once a week (1)
_____ 3 or more times per week (5)
How often do you experience constipation or stools that are compact or hard to pass?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 or more times per week (5)
Do you find that you often burp after meals?
_____ Yes (3)
_____ No (0)
Do you frequently have gas?
_____ Yes (3)
_____ No (0)
Do you crave certain foods such as bread, chocolate, certain fruit, and red meat if you have not eaten them in a day or two?
_____ Yes (5)
_____ No (0)
How often do you have a poor appetite or feel worse after eating?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 times per week (5)
_____ 3 or more times per week (10)
Do you have an excessive appetite and/or sweet cravings?
_____ Yes (5)
_____ No (0)
Do you frequently (more than twice a week) experience abdominal pain, cramps or general abdominal discomfort?
_____ Yes (20)
_____ No (0)
How often do you have indigestion, heartburn or an upset stomach?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 times per week (5)
_____ 3 or more times per week (10)
How often do you get a headache after eating?
_____ Never or very rarely (0)
_____ 1-2 times per week (3)
_____ 3 or more times per week (5)
Fungus & Parasites
Have you ever been given general anesthesia?
_____ Yes (10)
_____ No (0)
Have you ever taken antibiotics?
_____ Yes (10)
_____ No (0)
Have you been or are you being treated for any condition requiring that you take medical drugs?
_____ Yes (10)
_____ No (0)
In general, are your bowel movements loose, hard or foul smelling?
_____ Yes (10)
_____ No (0)
Would you consider your life to be:
_____ Stress free (0)
_____ Mildly stressful (5)
_____ Very stressful (10)
Do you currently suffer from any digestive disorder or frequently have pain in the region above or below the navel?
_____ Yes (10)
_____ No (0)
Do you have mercury amalgam fillings in your mouth?
_____ Yes (10)
_____ No (0)
Do you have two different kinds of metal in your mouth; i.e., gold and silver or mercury amalgam and gold or silver?
_____ Yes (5)
_____ No (0)
Do you experience itching in the ears, nose or rectum area?
_____ Yes (10)
_____ No (0)
Do you have or have you had dandruff in the past year?
_____ Yes (10)
_____ No (0)
Do you regularly eat or drink products containing sugar, white flour, processed dairy products?
_____ Yes (5)
_____ No (0)
Do you crave sugar, fruit or milk if you don't have either of these items for more than three days?
_____ Yes (10)
_____ No (0)
Do you find that regardless of how much you eat you get hungry quickly?
_____ Yes (5)
_____ No (0)
In the past year, have you experienced athlete's foot (itching around the toes, soles or heel of the feet), jock itch or a fungal infection under a toenail (thickening of the toenail)?
_____ Yes (20)
_____ No (0)
Do you ever get a reddening around the mouth or nose area after eating or drinking?
_____ Yes (5)
_____ No (0)
Do you experience muscle or joint aches on a regular basis?
_____ Yes (5)
_____ No (0)
Do you experience mood swings?
_____ Yes (10)
_____ No (0)
Do you snack on sweets or drink coffee, soda pop or sports drinks most days to keep your energy up?
_____ Yes (10)
_____ No (0)
Do you suffer from any kind of skin condition?
_____ Yes (10)
_____ No (0)
Have you ever had sex or close physical contact with anyone who you know had a fungal infection (including athletes foot, jock itch, dandruff) or parasite infection?
_____ Yes (20)
_____ No (0)
_____ Yes (10)
_____ No (0)
Have you ever taken antibiotics?
_____ Yes (10)
_____ No (0)
Have you been or are you being treated for any condition requiring that you take medical drugs?
_____ Yes (10)
_____ No (0)
In general, are your bowel movements loose, hard or foul smelling?
_____ Yes (10)
_____ No (0)
Would you consider your life to be:
_____ Stress free (0)
_____ Mildly stressful (5)
_____ Very stressful (10)
Do you currently suffer from any digestive disorder or frequently have pain in the region above or below the navel?
_____ Yes (10)
_____ No (0)
Do you have mercury amalgam fillings in your mouth?
_____ Yes (10)
_____ No (0)
Do you have two different kinds of metal in your mouth; i.e., gold and silver or mercury amalgam and gold or silver?
_____ Yes (5)
_____ No (0)
Do you experience itching in the ears, nose or rectum area?
_____ Yes (10)
_____ No (0)
Do you have or have you had dandruff in the past year?
_____ Yes (10)
_____ No (0)
Do you regularly eat or drink products containing sugar, white flour, processed dairy products?
_____ Yes (5)
_____ No (0)
Do you crave sugar, fruit or milk if you don't have either of these items for more than three days?
_____ Yes (10)
_____ No (0)
Do you find that regardless of how much you eat you get hungry quickly?
_____ Yes (5)
_____ No (0)
In the past year, have you experienced athlete's foot (itching around the toes, soles or heel of the feet), jock itch or a fungal infection under a toenail (thickening of the toenail)?
_____ Yes (20)
_____ No (0)
Do you ever get a reddening around the mouth or nose area after eating or drinking?
_____ Yes (5)
_____ No (0)
Do you experience muscle or joint aches on a regular basis?
_____ Yes (5)
_____ No (0)
Do you experience mood swings?
_____ Yes (10)
_____ No (0)
Do you snack on sweets or drink coffee, soda pop or sports drinks most days to keep your energy up?
_____ Yes (10)
_____ No (0)
Do you suffer from any kind of skin condition?
_____ Yes (10)
_____ No (0)
Have you ever had sex or close physical contact with anyone who you know had a fungal infection (including athletes foot, jock itch, dandruff) or parasite infection?
_____ Yes (20)
_____ No (0)
Score Sheet
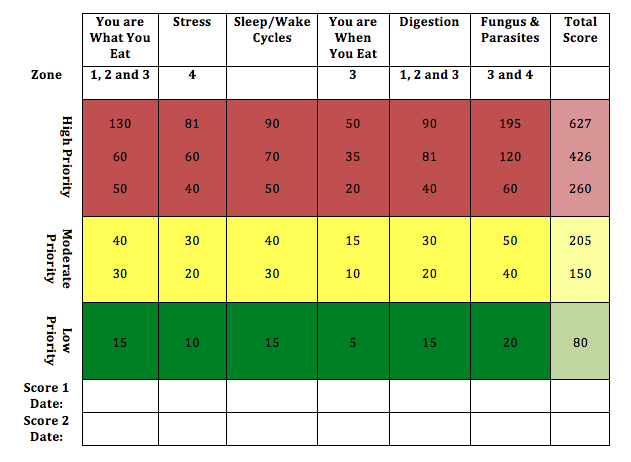
Image by Joe Pineda
| Nutrition and Lifestyle Questionnaires.docx |
References
Chek, P. (2004). How to eat, move and be healthy. San Diego, CA.: C.H.E.K Institute.





