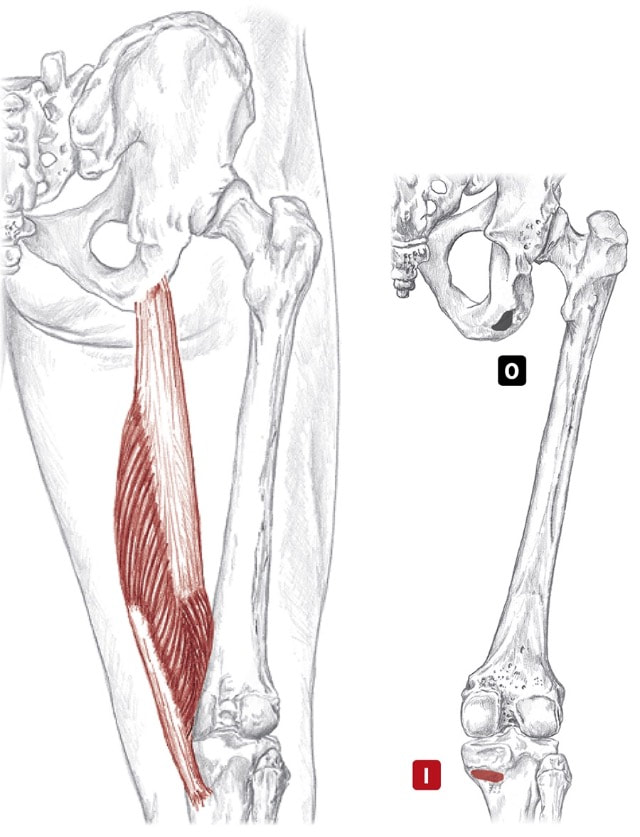
 Posterior views of right hip and thigh. (image by R. Dorn) sem-eye-mem-bra-no-sus Action
Origin
Insertion
Nerve
Hamstrings as a group Location: Superficial, posterior thigh BLMs: Ischial tuberosity, tendons of posterior knee Action: "Bend your knee" or "extend your hip"
0 Comments
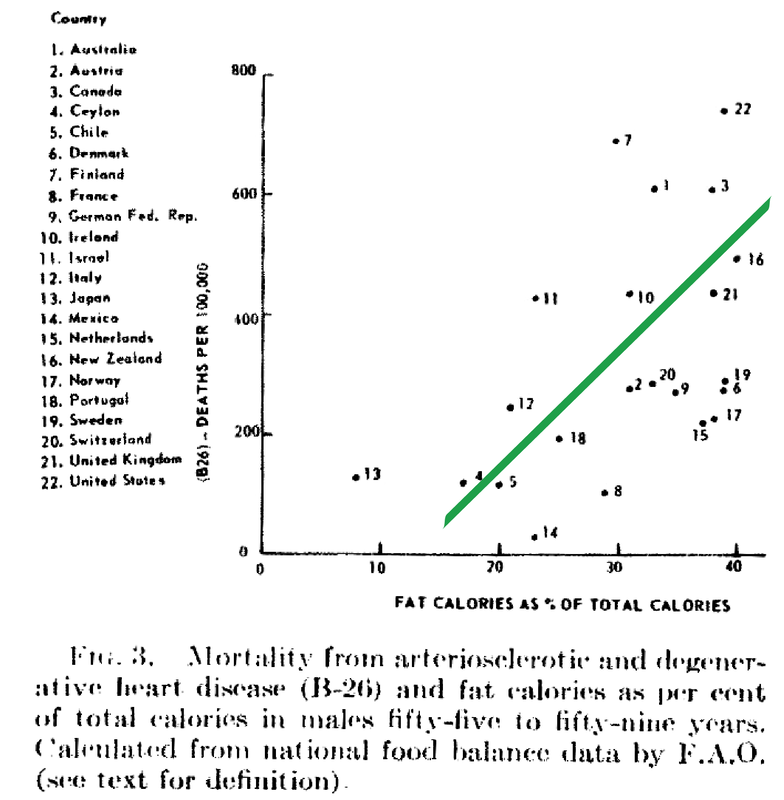
Despite food manufacturers claiming that refined vegetable oils were healthy, Americans experienced an up-rise in heart disease during the early 20th century. Like many new inventions, few questions were initially posited. Unfortunately, an alternate nutrient took the blame due to the research of a single scientist. In 1951, American physiologist and professor Ancel Keys went to Europe in search of the cause of cardiovascular disease. In his quest, he went to observe the eating habits of individuals living Naples, Italy due to reports of a low prevalence of heart disease. During this time, post-war conditions resulted in finite and unusual circumstances in regards to agriculture and infrastructure. Therefore what Keys perceived as a cultural tradition was dubbed the "Mediterranean diet". Keys observed the residents in Naples consumed primarily pasta and plain pizza, with vegetables, olive oil, cheese, fruit for dessert, a moderate amount of wine, and very little meat (except among individuals belonging to a higher socioeconomic status).  Through an informal study measuring cholesterol serum levels among Rotary club members (those who could not afford meat, but could afford cheese) conducted by Keys's wife, whom at the time was a medical technologist, Keys deduced that avoiding meat resulted in a lower incidence of heart attacks. Ancel Keys continued on his biased search for proof that a diet high in saturated fat is correlated with a higher risk of cardiovascular disease. He eventually compiled data from six more countries with high rates of heart disease and diets typically high in saturated fat. At first glance, Keys's research seemed logical and compelling. The evidence was based on the premise that individuals in America, who consumed high amounts of saturated fat, died from heart disease at a higher rate than individuals in Japan, who consumed low amounts of saturated fat.
Unfortunately, Keys had gained the interest of people in positions of power. Upon President Eisenhower's heart attack in 1955, Keys proposed his theory to the president's primary care physician, Paul Dudley White. Days following, White began to advise to the public to reduce the consumption of saturated fat and cholesterol in an effort to prevent cardiovascular disease. Through his connections and influence, Keys soon joined the nutrition committee of the American Heart Association (AHA) which, based on Keys's research, released a report in 1961 that advised patients with a high risk of cardiovascular disease to reduce their consumption of saturated fat. (Interestingly enough, the AHA began its rise to prominence in 1948, the same year Proctor & Gamble donated over $1.7 million to the organization - resulting in the AHA indebted to Crisco.) In 1961, Time magazine placed Ancel Keys on the front cover touting him as "the twenthiest century's most influential nutrition expert." By 1970, Keys published the Seven Countries Study, which detailed his original research - this study has now been cited in over a million other scientific publications. While Keys associative observations between saturated fat and cardiovascular disease never proved causation, he had won the battle of public opinion. With the help of Ancel Keys, the American medical community and mainstream media has advised consumers to stop eating the animal products that have been consumed for centuries, replacing them with bread, pasta, margarine, low-fat dairy, and vegetable oil. This was the dietary shift that was codified by the United States government in the late 1970s. References Central Committee for Medical And Community Program of the American Heart Association. (1961). Dietary Fat and Its Relation to Heart Attacks and Strokes. Circulation [online] 23, pp.133-36. Available at: https://circ.ahajournals.org/content/circulationaha/23/1/133.full.pdf [Accessed 26 Jan. 2019]
Keys, A. (1953). Atherosclerosis: A Problem in Newer Public Health. Journal of Mt. Sinai Hospital, [online] 20(2), pp.118-39. Keys, A. (1970). Coronary Heart Disease in Seven Countries. Circulation. 41 (1), pp.1186-95. Keys, A. (1995). Mediterranean Diet and Public Health: Personal Reflections. American Journal of Clinical Nutrition, [online] 61 (6), pp.1321S-1323S. Available at: https://dx.doi.org/10.1093/ajcn/61.6.1321s [Accessed 26 Jan. 2019] Marvin, H. (1964). The 40 Year War on Heart Disease. New York: American Heart Association. Mercola, J. (2017). Fat For Fuel. Carlsbad, California: Hay House. Teichholz, N. (2014). The Big Fat Surprise. New York: Simon & Schuster, pp.32-33. 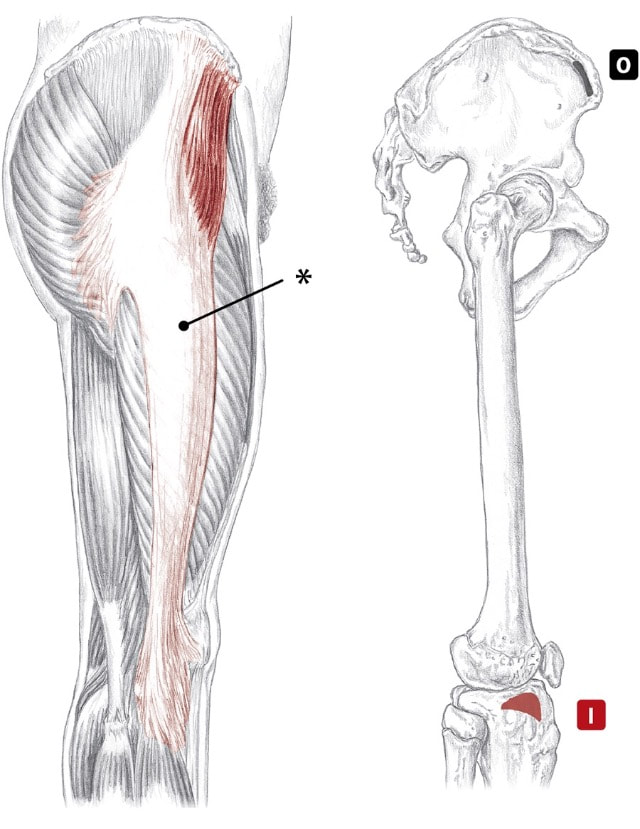 Lateral views of right hip and thigh, right illustration showing origin of TFL and insertion of iliotibial tract. (Image by R. Dorn) ten-sor fash-ay la-ta Action
Origin
Insertion
Nerve
Location: Superficial BLMs: ASIS, iliac crest and iliotibial tract Action: "Medially rotate your hip" The environment that we live in is toxic. It is worrisome to think that the status quo has occurred with the help of corporations knowingly dumping harmful chemicals into the environment.
The Environmental Working Group (EWG) has studied the current state of our world in great detail and has discovered that before a child is even born they already have approximately 287 toxins in their blood and tissues. These results came from 10 newborns whose parents gave permission to have their toxins measured at birth. The results of this study indicate that an average of 200 chemicals was found in each newborn. Of the toxins tested, 47 were consumer ingredients such as cosmetics, 212 were industrial and pesticide byproducts. In this study, only around 400 total chemicals were actually tested for - thousands of others may have been found if larger parameters were used. Many of the toxins measured in the newborns included plastics, flame retardants, and other chemicals that disrupt brain function, IQ, hormones, and the nervous system of the child. Some of the toxins observed like DDT, have actually been banned since 1972 (over 3 decades ago), but are still being measured in laboratory samples. Certain chemicals never fully degrade in the environment. So, there is not question about it, the environment we live in is toxic. All of us have disease-creating toxins inside of our bodies, the question boils down to which ones and how much. But there are some solutions: lab tests and detoxification. 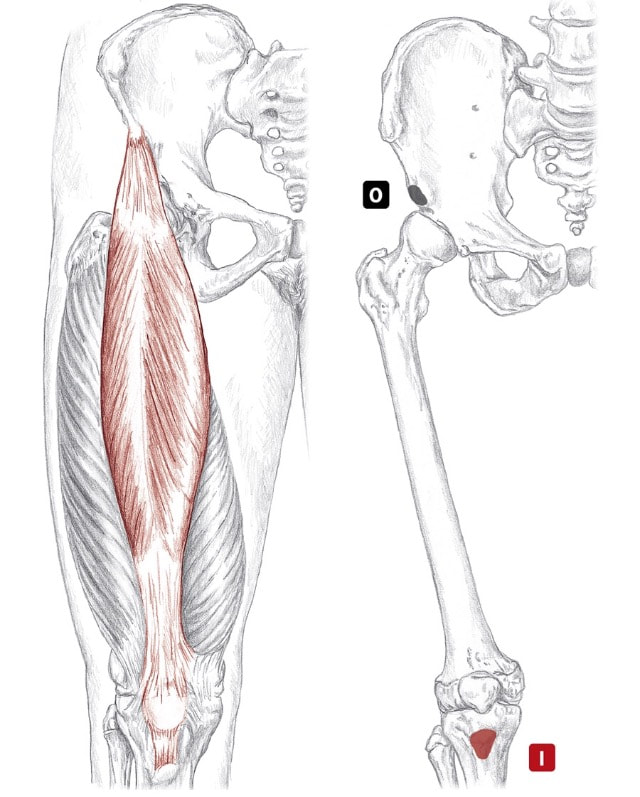 Anterior views of right hip and thigh. (Image by R. Dorn) rek-tus fe-mo-ris Action
Origin
Insertion
Nerve
Quadriceps as a group Location Superficial, anterior and lateral thigh BLMs Patella, tibial tuberosity Action "Straighten your knee" or "flex your hip" 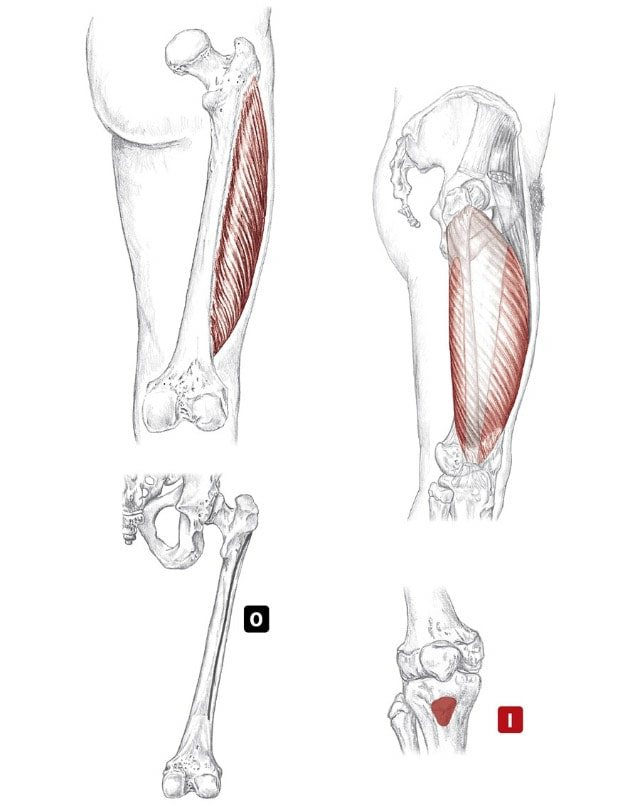 Posterior and medial views of right hip and thigh, bottom right showing anterior view of tibiofemoral joint. (Image by R. Dorn) vas-tus lat-er-a-lis Action
Origin
Insertion
Nerve
Quadriceps as a group Location Superficial, anterior and lateral thigh BLMs Patella, tibial tuberosity Action "Straighten your knee" or "flex your hip" 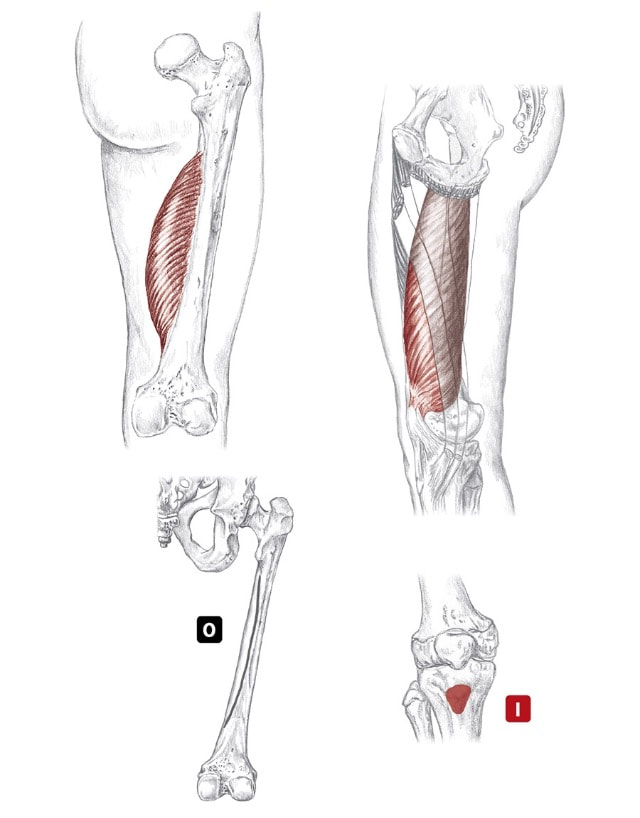 Posterior and medial views of right hip and thigh, bottom right showing anterior view of tibiofemoral joint. (Image by R. Dorn) vas-tus me-dee-a-lis Action
Origin
Insertion
Nerve
Quadriceps as a group Location Superficial, anterior and lateral thigh BLMs Patella, tibial tuberosity Action "Straighten your knee" or "flex your hip" 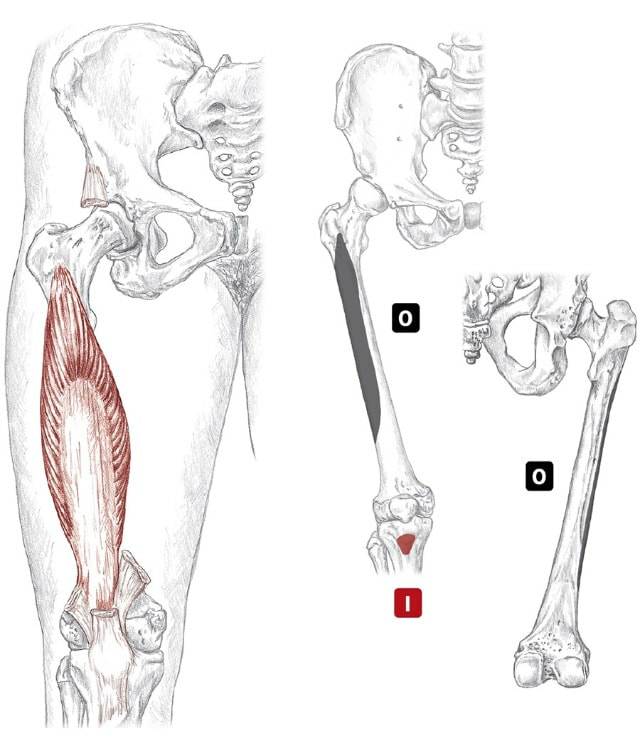 Anterior and posterior views of right hip and thigh. (Image by R. Dorn) vas-tus in-ter-me-dee-us Action
Origin
Insertion
Nerve
Quadriceps as a group Location Superficial, anterior and lateral thigh BLMs Patella, tibial tuberosity Action "Straighten your knee" or "flex your hip" Dr. Sharon Goldberg, an internal medicine physician and professor gives her testimony at Michigan's 5G Small Cell Tower Legislation Hearing on October 4, 2018 regarding the dangers of electromagnetic radiation.
She says: "Wireless radiation has biological effects. Period. This is no longer a subject for debate when you look at PubMed and the peer-review literature. These effects are seen in all life forms; plants, animals, insects, microbes. In humans we have clear evidence of cancer now; there is no question. We have evidence of DNA damage, cardiomyopathy, which is the precursor of congestive heart failure, neuropsychiatric effects... 5G is an untested application of a technology that we know is harmful; we know it from the science. In academics this is called human subjects research." 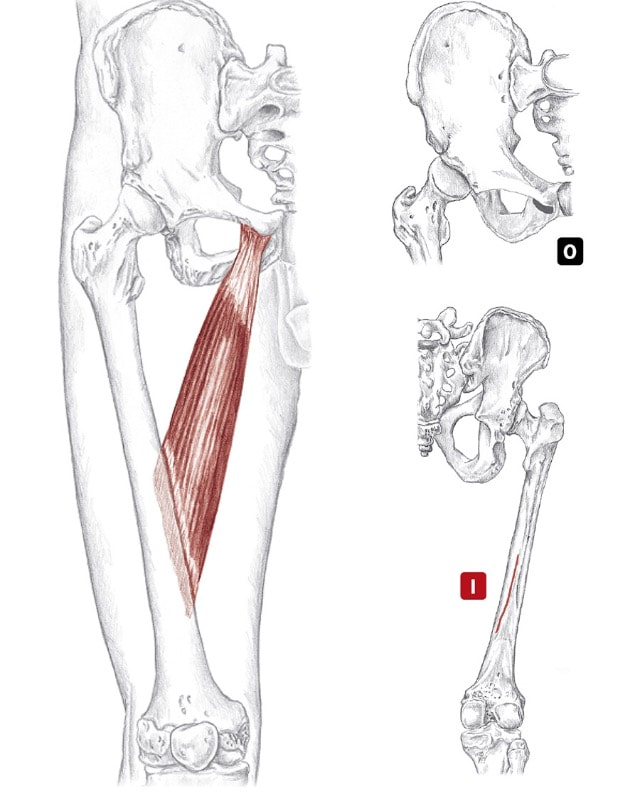 Anterior and posterior views of right hip and thigh. (Image by R. Dorn) ad-duk-ter long-us Action
Origin
Insertion
Nerve
Adductor group Location: Superficial and deep, medial thigh BLMs: Pubic tubercle, rami and ischial tuberosity Action: "Squeeze your thighs together" 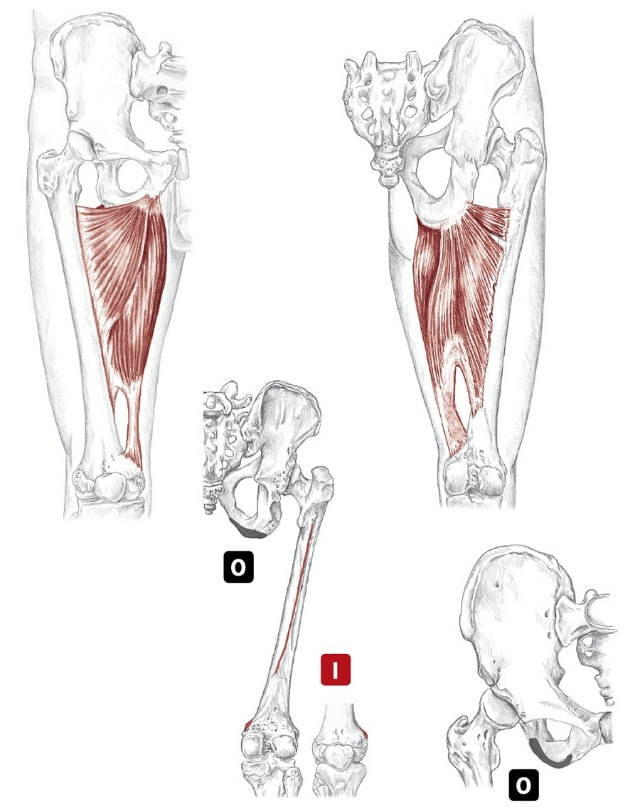 Anterior and posterior views of right thigh and hip. (Image by R. Dorn) ad-duk-ter mag-nus Action
Origin
Insertion
Nerve
Adductor group Location: Superficial and deep, medial thigh BLMs: Pubic tubercle, rami and ischial tuberosity Action: "Squeeze your thighs together" 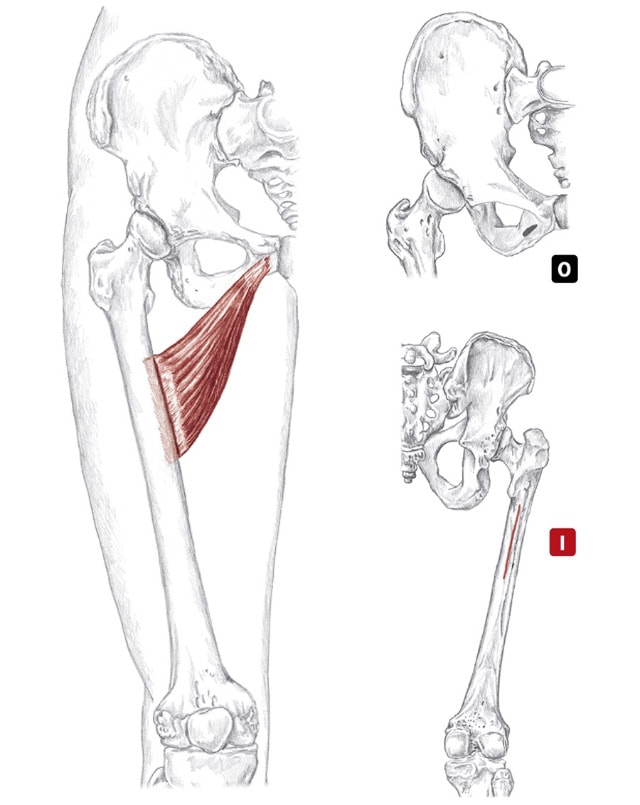 Anterior and posterior views of right hip and thigh. (Image by R. Dorn) ad-duk-ter breh-vis Action
Origin
Insertion
Nerve
Adductor group Location: Superficial and deep, medial thigh BLMs: Pubic tubercle, rami and ischial tuberosity Action: "Squeeze your thighs together" 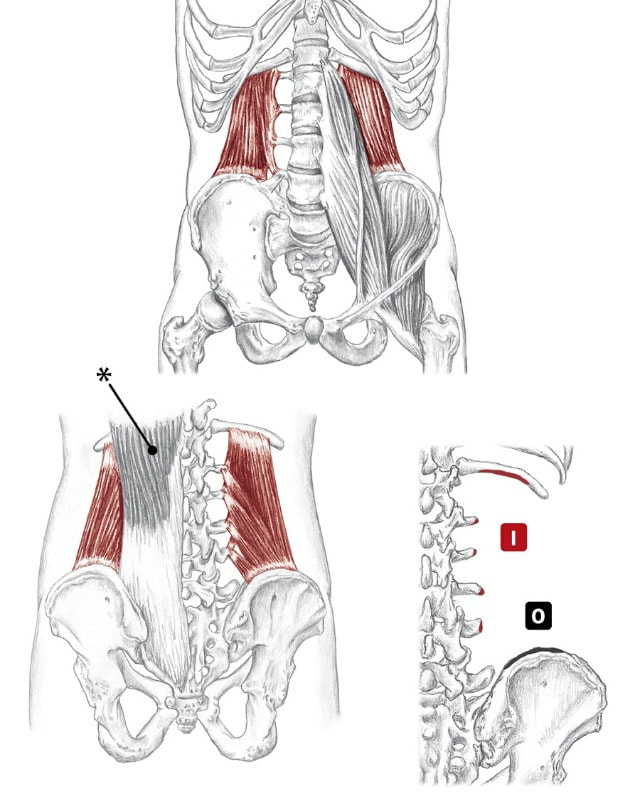 Anterior and posterior views. (Image by R. Dorn) kwod-rait-us lum-bor-um Action Unilaterally:
Origin
Insertion
Nerve
Location: Deep to erectors, low back BLMs: Twelfth rib and posterior iliac crest Action: "Hike your hip toward your shoulder" 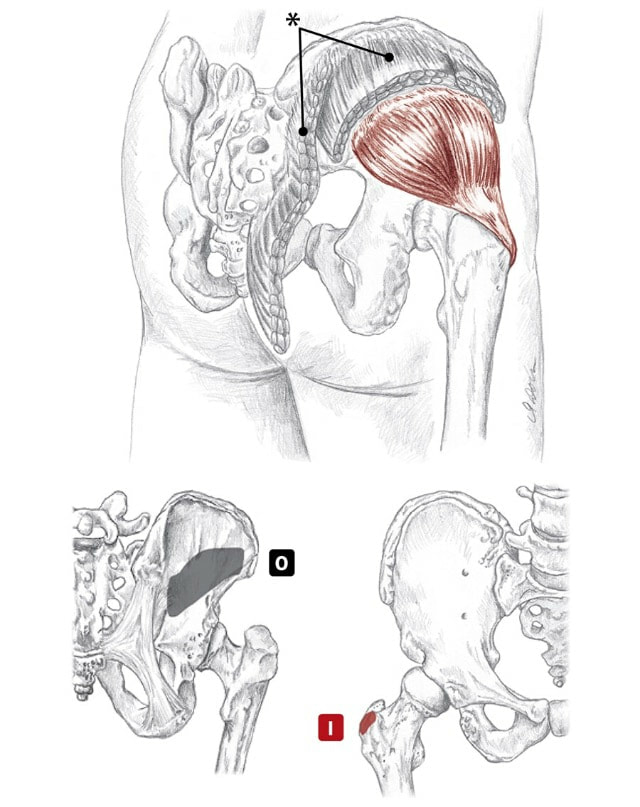 Posterior/lateral view of right buttock (top), posterior and anterior views (bottom). (Image by R. Dorn) gloo-te-us Action
Origin
Insertion
Nerve
Location: Deep to gluteus medius BLMs: Greater trochanter, gluteus medius Action: "Abduct your hip" 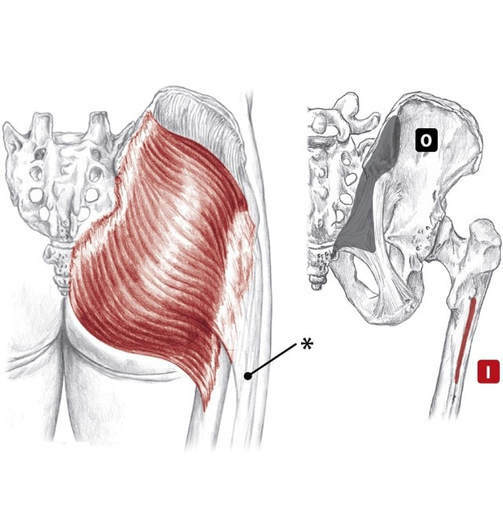 Posterior views of right buttock. (Image by R. Dorn) gloo-te-us Action All fibers:
Origin
Insertion
Nerve
Location: Superficial, posterior hip BLMs: Edge of sacrum, gluteal tuberosity Action: "Extend your hip" 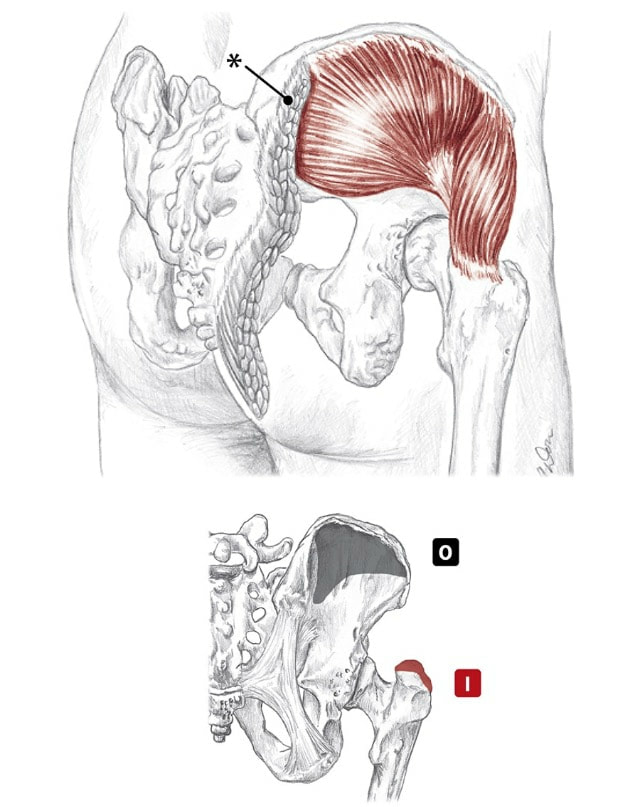 Posterior/lateral and posterior views of right buttock. (Image by R. Dorn) gloo-te-us Action All fibers:
Origin
Insertion
Nerve
Location: Partially superficial, lateral hip BLMs: Iliac crest, greater trochanter Action: "Abduct your hip" 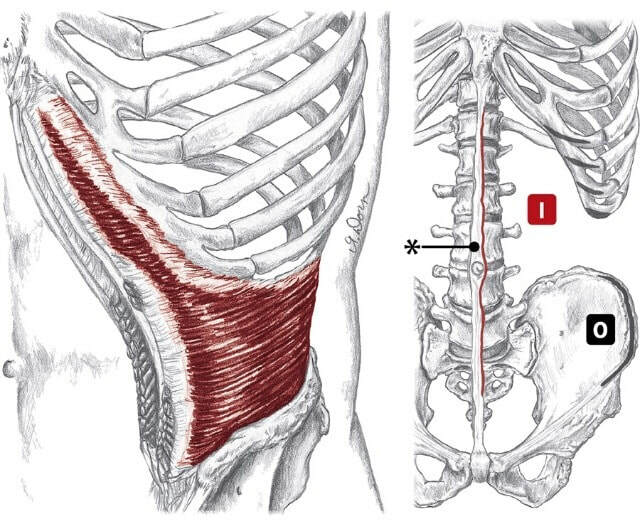 Anterior views. * Linea alba (Image by R. Dorn) ab-dah-min-is Action
Origin
Insertion
Nerve
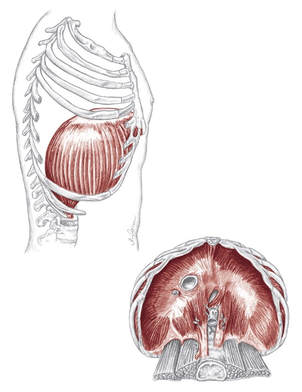 Lateral and inferior view of Diaphragm. (Image by R. Dorn) di-a-fram Action
Origin
Insertion
Nerve
Location: Underside of the ribs BLMs: Bottom edge of rib cage Action: "Inhale into your belly" A leading cardiovascular research scientist upends the low-salt myth, proving that salt may be one solution to—rather than a cause of—our nation’s chronic disease crises. Sure to change the national conversation about this historically treasured substance, The Salt Fix elegantly and accessibly weaves the research into a fascinating new understanding of salt’s essential role in your health and what happens when you aren’t getting enough—with far-reaching, even heart-stopping, implications. We’ve all heard the recommendation: eat no more than a teaspoon of salt a day for a healthy heart. But there’s one big problem with this: the vast majority of us don’t need to eat low-salt diets. In fact, for most of us, more salt would be better for our health, rather than less. (Not to mention, much tastier.) Scientific research suggests that the optimal range for sodium intake is 3 to 6 grams per day (about 1 ⅓ - 2 ⅔ teaspoons of salt) for healthy adults. Now, Dr. James DiNicolantonio reveals the incredible, often baffling story of how salt became unfairly demonized—a never-before-told, century-spanning drama of competing egos and interests. Not only have we gotten it wrong, we’ve gotten it exactly backwards: eating more salt can help protect you from a host of ailments, including internal starvation, insulin resistance, diabetes, and even heart disease. (The real culprit? Another white crystal—sugar.) Dr. DiNicolantonio in The Salt Fix shows how eating the right amount of this essential mineral will help you beat sugar cravings, achieve weight loss, improve athletic performance, increase fertility, and thrive with a healthy heart. James J. DiNicolantonio, Pharm. D., is a respected cardiovascular research scientist, doctor of pharmacy at Saint Luke's Mid America Heart Institute in Kansas City, Missouri, and the associate editor of British Medical Journal's (BMJ) Open Heart. He is the author or coauthor of approximately 200 publications in medical literature. His research has been featured in The New York Times, ABC’s Good Morning America, TIME, Fox News, U.S. News and World Report, Yahoo! Health, BBC News, Daily Mail, Forbes, National Public Radio, and Men’s Health, among others.  Welcome to the first episode of our brand new docuseries - Remedy: Ancient Medicine for Modern Illness.
(If you are not registered for the full Remedy docuseries yet, click this link to join us for all 9 episodes - https://remedy.thesacredscience.com/r... ) Episode 1 is called “The Quest For Lost Medicine” and it lays the groundwork for the entire series - some of what you will witness may shock you… Over the 9-part Remedy series, we’ll be uncovering powerful herbal remedies for major diseases - but first, we need to understand why this vital healing information has been kept from us. Here’s some of what we will reveal in this first episode…
This eye-opening episode sets the stage for everything else we cover in the Remedy docuseries. Again, if you are not registered for the full series, click here - https://remedy.thesacredscience.com/r... Top Cancer Researcher Fails to Disclose Corporate Financial Ties in Major Research Journals9/8/2018
The researcher, Dr. José Baselga, a towering figure in the cancer world, is the chief medical officer at Memorial Sloan Kettering Cancer Center in New York. He has held board memberships or advisory roles with Roche and Bristol-Myers Squibb, among other corporations, has had a stake in start-ups testing cancer therapies, and played a key role in the development of breakthrough drugs that have revolutionized treatments for breast cancer. According to an analysis by The New York Times and ProPublica, Dr. Baselga did not follow financial disclosure rules set by the American Association for Cancer Research when he was president of the group. He also left out payments he received from companies connected to cancer research in his articles published in the group’s journal, Cancer Discovery. At the same time, he has been one of the journal’s two editors in chief. At a conference this year and before analysts in 2017, he put a positive spin on the results of two Roche-sponsored clinical trials that many others considered disappointments, without disclosing his relationship to the company. Since 2014, he has received more than $3 million from Roche in consulting fees and for his stake in a company it acquired. Dr. Baselga did not dispute his relationships with at least a dozen companies. In an interview, he said the disclosure lapses were unintentional. He stressed that much of his industry work was publicly known although he declined to provide payment figures from his involvement with some biotech startups. “I acknowledge that there have been inconsistencies, but that’s what it is,” he said. “It’s not that I do not appreciate the importance.” Dr. Baselga’s extensive corporate relationships — and his frequent failure to disclose them — illustrate how permeable the boundaries remain between academic research and industry, and how weakly reporting requirements are enforced by the medical journals and professional societies charged with policing them. A decade ago, a series of scandals involving the secret influence of the pharmaceutical industry on drug research prompted the medical community to beef up its conflict-of-interest disclosure requirements. Ethicists worry that outside entanglements can shape the way studies are designed and medications are prescribed to patients, allowing bias to influence medical practice. Disclosing those connections allows the public, other scientists and doctors to evaluate the research and weigh potential conflicts. “If leaders don’t follow the rules, then we don’t really have rules,” said Dr. Walid Gellad, director of the Center for Pharmaceutical Policy and Prescribing at the University of Pittsburgh. “It says that the rules don’t matter.” The penalties for such ethical lapses are not severe. The cancer research group, the A.A.C.R., warns authors who fill out disclosure forms for its journals that they face a three-year ban on publishing if they are found to have financial relationships that they did not disclose. But the ban is not included in the conflict-of-interest policy posted on its website, and the group said no author had ever been barred. Many journals and professional societies do not check conflicts and simply require authors to correct the record. Officials at the A.A.C.R., the American Society of Clinical Oncology and The New England Journal of Medicine said they were looking into Dr. Baselga’s omissions after inquiries from The New York Times and ProPublica. The Lancet declined to say whether it would look into the matter. Christine Hickey, a spokeswoman for Memorial Sloan Kettering, said that Dr. Baselga had properly informed the hospital of his outside industry work and that it was Dr. Baselga’s responsibility to disclose such relationships to entities like medical journals. The cancer center, she said, “has a rigorous and comprehensive compliance program in place to promote honesty and objectivity in scientific research.” Asked if he planned to correct his disclosures, Dr. Baselga asked reporters what they would recommend. In a statement several days later, he said he would correct his conflict-of-interest reporting for 17 articles, including in The New England Journal of Medicine, The Lancet and the publication he edits, Cancer Discovery. He said that he did not believe disclosure was required for dozens of other articles detailing early stages of research. “I have spent my career caring for cancer patients and bringing new therapies to the clinic with the goal of extending and saving lives,” Dr. Baselga said in the statement. “While I have been inconsistent with disclosures and acknowledge that fact, that is a far cry from compromising my responsibilities as a physician, as a scientist and as a clinical leader.” The corporate imprint on cancer researcher Dr. Baselga, 59, supervises clinical operations at Memorial Sloan Kettering, one of the nation’s top cancer centers, and wields influence over the lives of patients and companies wishing to conduct trials there. He was paid more than $1.5 million in compensation by the cancer center in 2016, according to the hospital’s latest available tax disclosures, but that does not include his consulting or board fees from outside companies. Many top medical researchers have ties to the for-profit health care industry, and some overlap is seen as a good thing — after all, these are the companies charged with developing the drugs, medical devices and diagnostic tests of the future. Dr. Baselga’s relationship to industry is extensive. In addition to sitting on the board of Bristol-Myers Squibb, he is a director of Varian Medical Systems, which sells radiation equipment and for whom Memorial Sloan Kettering is a client. In all, Dr. Baselga has served on the boards of at least six companies since 2013, positions that have required him to assume a fiduciary responsibility to protect the interests of those companies, even as he oversees the cancer center’s medical operations. The hospital and Dr. Baselga said steps had been taken to prevent him from having a say in any business between the cancer center and the companies on whose boards he sits. The chief executive of Memorial Sloan Kettering, Dr. Craig B. Thompson, settled lawsuits several years ago that were filed by the University of Pennsylvania and an affiliated research center. They contended that he hid research conducted while he was at Penn to start a new company, Agios Pharmaceuticals, and did not share the earnings. Dr. Thompson disputed the allegations. He now sits on the board of Merck, which manufactures Keytruda, a blockbuster cancer therapy. Ms. Hickey said the cancer center cannot fulfill its charitable mission without working with industry. “We encourage collaboration and are proud that our work has led to the approval of novel, lifesaving cancer treatments for patients around the world,” she said. Some disclosures are required; others aren’t. After the scandals a decade ago over lack of disclosure, the federal government began requiring drug and device manufacturers to publicly disclose payments to doctors in 2013. From August 2013 through 2017, Dr. Baselga received nearly $3.5 million from nine companies, according to the federal Open Payments database, which compiles disclosures filed by drug and device companies. Dr. Baselga has disclosed in other forums investments and advisory roles in biotech start-ups, but he declined to provide a tally of financial interests in those firms. Companies that have not received approval from the Food and Drug Administration for their products — projects still in the testing phases — do not have to report payments they make to doctors. Serving on boards can be lucrative. In 2017, he received $260,000 in cash and stock awards to sit on Varian’s board of directors, according to the company’s corporate filings. ProPublica and The Times analyzed Dr. Baselga’s publications in medical journals since 2013, the year he joined Memorial Sloan Kettering. He failed to disclose any industry relationships in more than 100, or about 60 percent of the time, a figure that has increased with each passing year. Last year, he did not list any potential conflicts in 87 percent of the articles that he wrote or co-wrote. Dr. Baselga compiled a color-coded list of his articles and offered a different interpretation. Sixty-two of the papers for which he did not disclose any potential conflict represented “conceptual, basic laboratory or translational work,” and did not require one, he said. Questions could be raised about others, he said, but he added that most “had no clinical nor financial implications.” That left the 17 papers he plans to correct. Early-stage research often carries financial weight because it helps companies decide whether to move ahead with a product. In about two-thirds of Dr. Balsega’s articles that lacked details of his industry ties, one or more of his co-authors listed theirs. In 2015, Dr. Baselga published an article in the New England Journal about a Roche-sponsored trial of one of the company’s drugs, Zelboraf. Despite his financial ties to Roche, he declared that he had “nothing to disclose.” Fourteen of his co-authors reported ties to Roche. Dr. Baselga defended the articles, saying that “these are high-quality manuscripts reporting on important clinical trials that led to a better understanding of cancer treatments.” Industry ConnectionsSome of Dr. José Baselga’s known relationships with health care companies. He has failed to disclose any industry ties in dozens of research articles since 2013.  The guidelines enacted by most major medical journals and professional societies ask authors and presenters to list recent financial relationships that could pose a conflict. But much of this reporting still relies on the honor system. A study in August in the journal JAMA Oncology found that one-third of authors in a sample of cancer trials did not report all payments from the studies’ sponsors. “We don’t routinely check because we don’t have those kind of resources,” said Dr. Rita F. Redberg, the editor of JAMA Internal Medicine, who has been critical of the influence of industry on medical practice. “We rely on trust and integrity. It’s kind of an assumed part of the professional relationship.” Jennifer Zeis, a spokeswoman for The New England Journal of Medicine, said in an email that it had now asked Dr. Baselga to amend his disclosures. She said the journal planned to overhaul its tracking of industry relationships. The American Association for Cancer Research said it had begun an “extensive review” of the disclosure forms submitted by Dr. Baselga. It said that it had never barred an author from publishing, and that “such an action would be necessary only in cases of egregious, consistent violations of the rules.” Among the most prominent relationships that Dr. Baselga has often failed to disclose is with the Swiss pharmaceutical giant Roche and its United States subsidiary Genentech. In June 2017, at the annual meeting of the American Society of Clinical Oncology in Chicago, Dr. Baselga spoke at a Roche-sponsored investor event about study results that the company had been counting on to persuade oncologists to move patients from Herceptin — which was facing competition from cheaper alternatives — to a combination treatment involving Herceptin and a newer, more expensive drug, Perjeta. The results were so underwhelming that Roche’s stock fell 5 percent on the news. One analyst described the results as a “lead balloon,” and an editorial in The New England Journal called it a “disappointment.” Dr. Baselga, however, told analysts that critiques were “weird” and “strange.” This June, at the same cancer conference, Dr. Baselga struck an upbeat note about the results of a Roche trial of the drug taselisib, saying in a blog post published on the cancer center website that the results were “incredibly exciting” while conceding the side effects from the drug were high. That same day, Roche announced it was scrapping plans to develop the drug. The news was another disappointment involving the class of drugs called PI3K inhibitors, which is a major focus of Dr. Baselga’s current research. In neither case did Dr. Baselga reveal that his ties to Roche and Genentech went beyond serving as a trial investigator. In 2014, Roche acquired Seragon, a cancer research company in which Dr. Baselga had an ownership stake, for $725 million. Dr. Baselga received more than $3 million in 2014 and 2015 for his stake in the company, according to the federal Open Payments database. From 2013 to 2017, Roche also paid Dr. Baselga more than $50,000 in consulting fees, according to the database. These details were not included in the conflict-of-interest statements that are required of all presenters at the American Society of Clinical Oncology conference, although he did disclose ownership interests and consulting relationships with several other companies in the prior two years. ASCO said it would conduct an internal review of Dr. Baselga’s disclosures and would refer the findings to a panel. Dr. Baselga said that he played no role in the Seragon acquisition, and that he had cut ties with Roche since joining the board of a competitor, Bristol-Myers, in March. As for his presentations at the ASCO meetings in the last two years, he said he had also noted shortcomings in the studies. The combination of Perjeta with Herceptin was later approved by the F.D.A. for certain high-risk patients. As for taselisib, Dr. Baselga stands by his belief that the PI3K class of drugs will be an important target for fighting cancer. ReferencesOrnstein, C & Thomas, K. (2018). Top Cancer Researcher Fails to Disclose Corporate Financial Ties in Major Research Journals. [online] Retrieved from: https://www.nytimes.com/2018/09/08/health/jose-baselga-cancer-memorial-sloan-kettering.html
What is the fastest way to health? It's simply honesty being honest with yourself. We each have four doctors within ourselves: Dr. Happiness, which is what is our concept of what makes us happy (what am you living for?); Dr. Quiet which is how do you create adequate rest to regenerate yourself to have a clear mind and to let my body recover from any stress; Dr. Diet (how do you tune into your body's particular nutritional needs?); and Dr. Movement, which is the difference between Working Out and Working In and putting those movement types to use in your life.
Wim Hof is an autodidact and taught himself how to control his heart rate, breathing and blood circulation. All this is regulated by the autonomic nervous system. Conventional science says that the autonomic nervous system is a part of the body you just can´t control, yet Wim can, by steering his hypothalamus (an area in the brain which regulates the body temperature). Where the body temperature of an untrained person drops dangerously after exposing it to extreme cold, Wim is able to retain his core temperature around 37 degrees Celsius, constantly. Even after 1 hour and 52 minutes sitting in ice, Wim’s core temperature stays the same. Scientists around the world baffled by this exceptional performance. In the Netherlands, Prof. Maria Hopman of the UMC St Radboud Nijmegen examined Wim’s physiology as he was affected by the cold, while he was up to his neck in a cylinder filled with ice cubes.
Wim Hof, aka "The Iceman" holds the world record for the longest ice bath lasting over one hour and 52 minutes and 20 other world records for feats performed while withstanding the cold. He has climbed Mount Everest and Mount Kilimanjaro in just shorts and shoes. His method enables him to control his core body temperature and immune system, which can be learned by anyone including. Wim's ultimate goals are to end all disease to facilitate a paradigm shift towards health to promote care for our planet and to bring back love and happiness for all people by encouraging them to get in touch with the cold, and he plans to do all this under the scrutiny of science. The anti-cancer assertions made by medical cannabis advocates are no longer just based on anecdotal success stories. In the following video, Dr. Christina Sanchez, a molecular biologist at the Complutense University of Madrid, explains how her research supports the claim that cannabis kills cancer. Through several human and animal experimental observations, researchers, such as Dr. Sanchez, have discovered that the application of the popular psychoactive compound found in cannabis, tetrahydrocannabinol (THC), has the potential to induce apoptosis in carcinogenic cells; in other words, THC kills cancer cells. This treatment significantly differs from other cancer treatments, such as chemotheraphy, because THC is able to distinguish between healthy and unhealthy cells, whereas chemotherapeutic agents cannot, resulting in a myriad of undesirable and deleterious side effects. According to Dr. Sanchez, "One of the advantages of cannabinoids, or cannabinoid based medicines, would be that they target a specifically, tumor cells. They don’t have any toxic effect on normal, non-tumoral cells. This is an advantage with respect to standard chemotherapy that target basically everything." Sanchez has further revealed that the cancer-killing effect of THC is potentiated by the presence of cannabidiol (CBD), a very potent antioxidant that protects the brain from stress and oxidative damage. These synergistic effects of both THC and CBD could make for a very safe and effective cancer concoction. Sanchez states, "I cannot understand why in the states cannabis is under schedule I, because it is pretty obvious not only from our work but from work from many other researchers that the plant has very wide therapeutic potential." Cannabinoids and the Endocannabinoid System The human body responds to the cannabinoids found in cannabis because it also makes its own endogenous cannabinoids. These endocannabinoids, which are lipid-based retrograde neurotransmitters that bind to cannabinoid receptors and proteins that are expressed throughout the mammalian central and peripheral nervous system, have been observed to mediate homeostasis via a variety of physiological and cognitive processes. This endocannabinoid system, named after the plant that led to its discovery, is a biological system of the body has many important regulatory functions affecting fertility, pregnancy, reproduction, appetite, pain-sensation, mood, locomotor behavior, exercise-induced euphoria, and memory. The endogenous cannabinoid system is perhaps the most important physiologic system involved in establishing and maintaining human health. Endocannabinoids and their receptors are found throughout the body: in the brain, organs, connective tissues, glands, and immune cells. In each tissue, the cannabinoid system performs different tasks, but the goal is always the same: homeostasis, the maintenance of a stable internal environment despite fluctuations in the external environment. A growing body of evidence continues to validate the miraculous healing capabilities of cannabinoids. Supporting the cultivation of cannabis and continued scientific research will lead to more availability of various cannabis strains specifically designed to have high doses and specific ratios of certain cannabinoids to serve as a safe and effective therapeutic treatment for a variety of disorders and diseases. The use of medical marijuana and cannabis-derived medicines in the treatment of diseases such as cancer, epilepsy, chronic pain, diabetes, multiple sclerosis, insomnia, depression, etc., will continue to grow. Cannabis may yet become one of the most useful natural remedies to some of the most crippling diseases of mankind. ReferencesHunt, Anna. (2018). Molecular Biologist Explains How Cannabis Kills Cancer Cells. [online] Waking Times. Available at: http://www.wakingtimes.com/2017/12/21/molecular-biologist-explains-cannabis-kills-cancer-cells/ [Accessed 6 Jul. 2018].
How much time do you spend sitting each day? Considering that excessive sedentary time is ubiquitous in Western societies, for most people, the total amount of time spent sitting could be cut in half, or even in quarters. "Sit less, move more" is the maxim worth repeating, especially with the growing body of evidence suggesting how detrimental prolonged sitting is for your body. A multitude of chronic metabolic diseases, including diabetes, obesity, cardiovascular disease, cancer, even premature death, have been directly associated with prolonged sitting time. According to several long-term studies, no matter how much you exercise, sitting for extended periods of time significantly increases your risk of disease and death, by any cause. The Relationship Between Sitting and Mortality Due to its prevalence, researchers set out to examine the association between daily, sedentary behavior (its total volume and accrual in prolonged, uninterrupted bouts) and all-cause mortality. Researchers shadowed nearly 8000 participants, age 45 or older, for an average of four years and observed that that sedentary behavior, on average, accounted for about 12.3 hours of an average 16-hour waking day. After analyzing the compiled data, the results of this observational experiment postulate a direct relationship; as total sedentary time increases, so does your risk of dying early than expected. Researchers have observed the participants' risk of metabolic morbidity and all-cause mortality grew in tandem with total sitting time and sitting stretch duration - no matter their age, sex, race, body mass index or exercise habits. In other words, prolonged sitting is a risk factor for all-cause mortality, independent of overall levels of moderate to vigorous physical activity. Furthermore, those who sat for more than 13 hours per day had a 2-fold (or 200%) greater risk of death compared to those who sat for less than about 11 hours per day (Diaz et al., 2017). The current exercise guidelines, established by the US Centers for Disease Control and Prevention, recommend adults perform moderate-intensity aerobic exercise for two hours and 30 minutes every week, plus resistance training exercises on two or more days a week. Even this recommendation, however, doesn’t address the importance of reducing sitting time in addition to increasing physical activity levels (Van der Ploeg, Chey, Korda, Banks & Bauman, 2012). Fortunately enough, the recommendations established by the researchers are, perhaps, more clear; take a movement break every 30 minutes. The researchers also determined that people who sit for less than 30 minutes at a time have the lowest risk of early death. According to the researchers, those who frequently sat in stretches less than 30 minutes had a 55% lower risk of death compared to people who usually sat for more than 30 minutes at a stretch. In addition, people who frequently sat for more than 90 minutes at a stretch had a nearly two-fold greater risk of death than those who almost always sat for less than 90 minutes at a stretch. If you have a job, obligation, or lifestyle where you have to sit for prolonged periods, the findings of this research recommend one behavior change could reduce your risk of death: take a movement break every 30 minutes While a standing desk might be helpful for those who work desk jobs, there is limited evidence to suggest that standing is a healthier alternative to sitting. Just taking a look at the anatomy of the human body, it is clear that it is designed for dynamic movement, not remain static. Each Hour Spent Sitting Decreases Your Life Expectancy by 2 hours In 2016, Dr. Mercola interviewed Kelly Starrett, who has a Ph.D. in physical therapy and is the author of "Deskbound: Standing Up to a Sitting World." In "Deskbound," Starrett quoted research from Dr. James Levine estimating for every hour you sit down, your life expectancy decreases by two hours. For comparison, every cigarette smoked reduces life expectancy by 11 minutes, which explains why some are now calling sitting the new smoking. For all intents and purposes, prolonged sitting may actually be far worse for your health than smoking. Starrett even mentioned a study that found office workers who smoked to be healthier than non-smokers simply because they got up every 30 minutes or so and walked outside to have a cigarette. In the end, it is clear that the human body is designed to move, and is not designed to stay in any fixed position. Take Away: Sitting and Standing are ToolsThe body is designed to move. Standing is not inherently better than sitting, and sitting is not inherently worse than standing - they are both tools. However from a metabolic perspective, standing is perhaps better, due to the relative rate of energy expenditure. Given this, it is not recommended to stand all day, or vice versa. What is most important, is how, or the way in which, you are sitting or standing. How is the quality of your sitting or standing position? How are utilizing your chair or the floor? If you are standing in an array of compromised positions, such as, for example, with an inwards collapsed knee or foot, or disengaged glutes, you are exacerbating the same patterns that result in physical discomfort. Sitting and standing are both tools, so it is important to ask yourself, "How am I using this tool?" To ensure proper posture, if you are going to be sitting, sit on the front edge of your seat, or the ischial tuberosity (the "sit bones" or bony protrusions located on your rear), with your hips located higher than your knees and your core activated. This position activates the spinal chain setting the sacrum and lumbar spine with a normal curve. If you are going to be standing, equally distribute the weight between your feet, stacking your spine while activating your glutes and core, with your shoulders back and down (not hunched forward), and your head neutral (not forward or looking down). References Diaz, K., Howard, V., Hutto, B., Colabianchi, N., Vena, J., Safford, M., Blair, S. and Hooker, S. (2017). Patterns of Sedentary Behavior and Mortality in U.S. Middle-Aged and Older Adults. Annals of Internal Medicine, 167(7), p.465. https://doi.org/10.7326/M17-0212
Scutti, S. (2018). Yes, sitting too long can kill you, even if you exercise. [online] CNN. Available at: https://www.cnn.com/2017/09/11/health/sitting-increases-risk-of-death-study/ [Accessed 31 May 2018]. Van der Ploeg, H., Chey, T., Korda, R., Banks, E. and Bauman, A. (2012). Sitting Time and All-Cause Mortality Risk in 222 497 Australian Adults. Archives of Internal Medicine, 172(6), p.494. https://doi.org/10.1001/archinternmed.2011.2174 |
The Awareness domain contains research, news, information, observations, and ideas at the level of self in an effort to intellectualize health concepts.
The Lifestyle domain builds off intellectual concepts and offers practical applications.
Taking care of yourself is at the core of the other domains because the others depend on your health and wellness.
Archives
April 2024
Categories
All
|


 RSS Feed
RSS Feed





